

Complement-targeted therapeutics
- PMID: 17989689
- PMCID: PMC2966895
- DOI: 10.1038/nbt1342
Complement-targeted therapeutics
Abstract
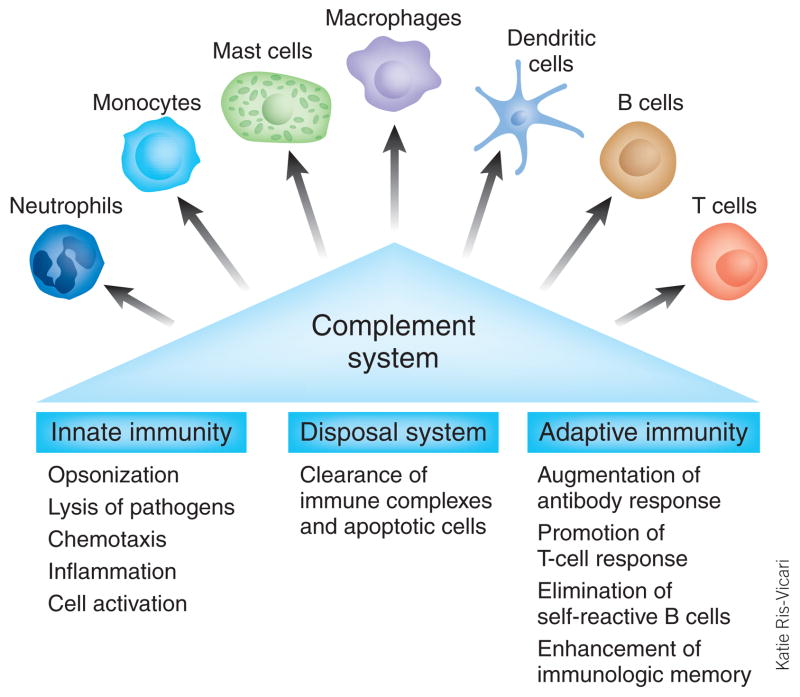
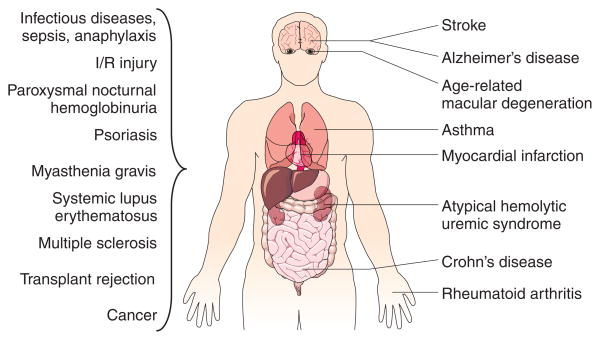
The complement system is a central component of innate immunity and bridges the innate to the adaptive immune response. However, it can also turn its destructive capabilities against host cells and is involved in numerous diseases and pathological conditions. Modulation of the complement system has been recognized as a promising strategy in drug discovery, and a large number of therapeutic modalities have been developed. However, successful marketing of complement-targeted drugs has proved to be more difficult than initially expected, and many strategies have been discontinued. The US Food and Drug Administration's approval of the first complement-specific drug, an antibody against complement component C5 (eculizumab; Soliris), in March 2007, was a long-awaited breakthrough in the field. Approval of eculizumab validates the complement system as therapeutic target and might facilitate clinical development of other promising drug candidates.
Conflict of interest statement
The authors declare competing financial interests: details accompany the full-text HTML version of the paper at
Figures
References
-
- Nuttall G. Experimente über die bacterienfeindlichen Einflüsse des thierischen Körpers. Z Hyg Infektionskr. 1888;4:353–394.
-
- Ehrlich P, Morgenroth J. Ueber haemolysine—zweite mittheilung. Berl Klin Wochenschr. 1899:481–486.
-
- US Food and Drug Administration. FDA approves first-of-its-kind drug to treat rare blood disorder. USFDA; Rockville, MD, USA: Mar 16, 2007. ( http://www.fda.gov/bbs/topics/NEWS/2007/NEW01589.html)
-
- Sunyer JO, Zarkadis IK, Lambris JD. Complement diversity: a mechanism for generating immune diversity? Immunol Today. 1998;19:519–523. - PubMed
-
- Walport MJ. Complement. First of two parts. N Engl J Med. 2001;344:1058–1066. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
