

Stability of cirrhotic systemic hemodynamics ensures sufficient splanchnic blood flow after living-donor liver transplantation in adult recipients with liver cirrhosis
- PMID: 17990357
- PMCID: PMC4205438
- DOI: 10.3748/wjg.v13.i44.5918
Stability of cirrhotic systemic hemodynamics ensures sufficient splanchnic blood flow after living-donor liver transplantation in adult recipients with liver cirrhosis
Abstract
Aim: To investigate the correlation between systemic hemodynamics and splanchnic circulation in recipients with cirrhosis undergoing living-donor liver transplantation (LDLT), and to clarify how systemic hemodynamics impact on local graft circulation after LDLT.
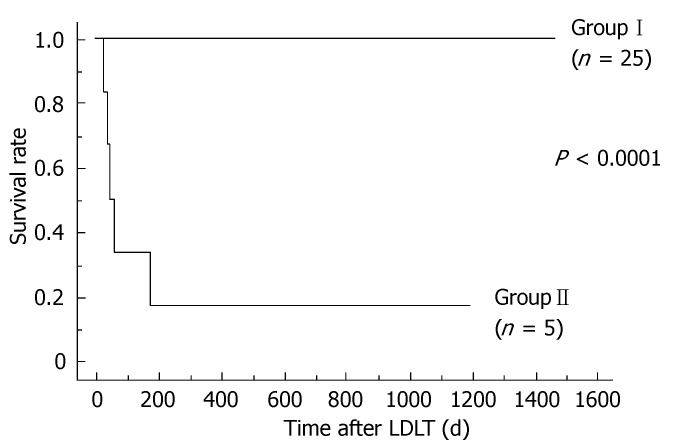
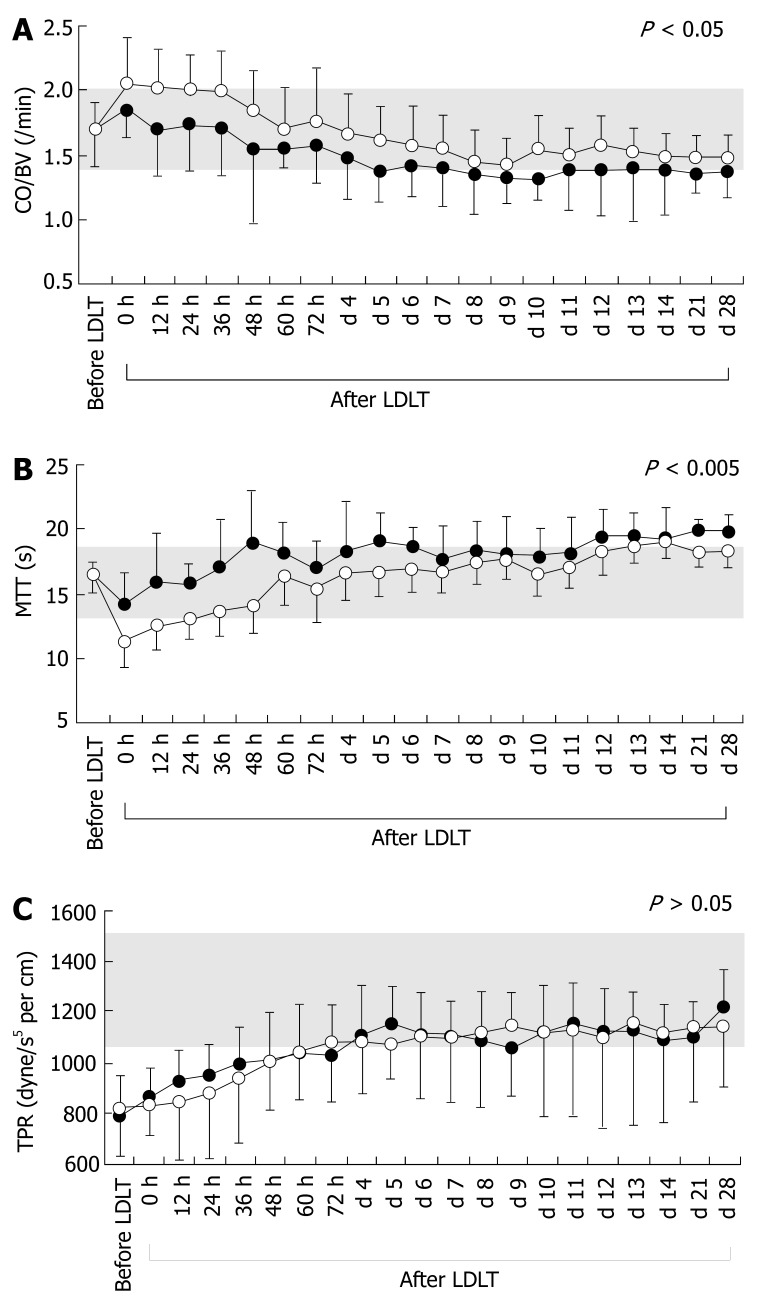
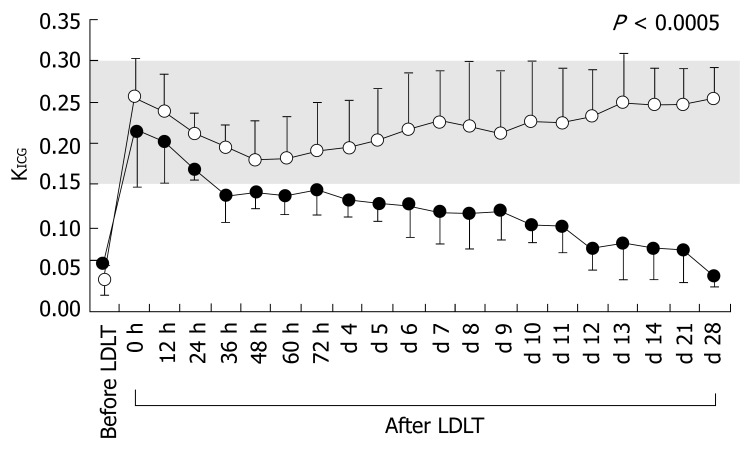
Methods: Systemic hemodynamics, indocyanine green (ICG) elimination rate (K ICG) and splanchnic circulation were simultaneously and non-invasively investigated by pulse dye densitometry (PDD) and ultrasound. Accurate estimators of optimal systemic hyperdynamics after LDLT [i.e., balance of cardiac output (CO) to blood volume (BV) and mean transit time (MTT), defined as the time required for half the administered ICG to pass through an attached PDD sensor in the first circulation] were also measured. Thirty recipients with cirrhosis were divided into two groups based on clinical outcomes corresponding to postoperative graft function.
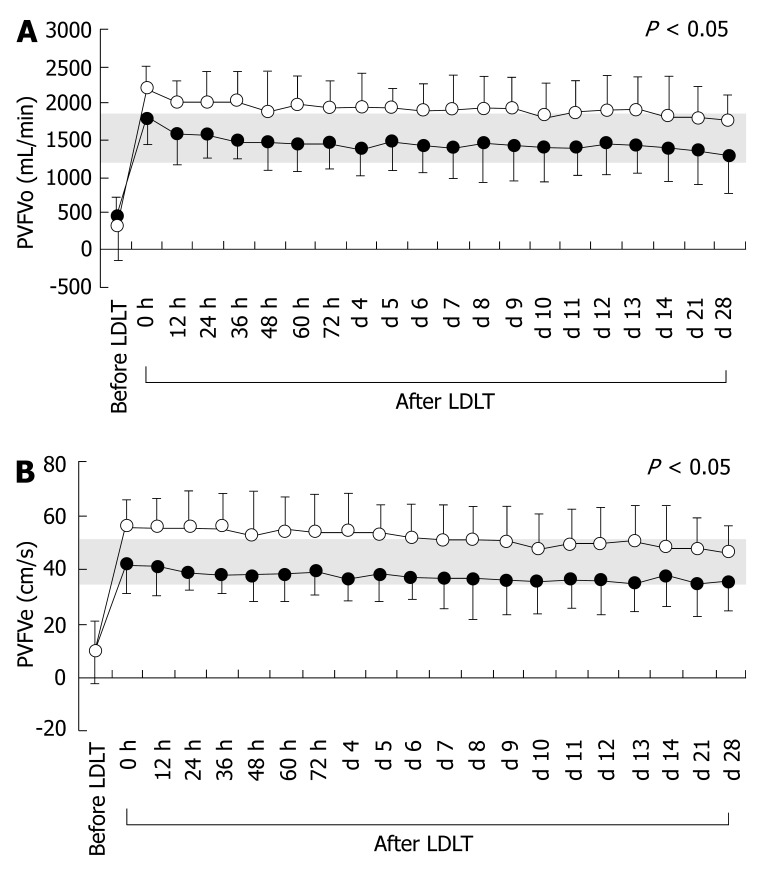
Results: Cirrhotic systemic hyperdynamics characterized by high CO, expanded BV and low total peripheral resistance (TPR) were observed before LDLT. TPR reflecting cirrhotic vascular alterations was slowly restored after LDLT in both groups. Although no significant temporal differences in TPR were detected between the two groups, CO/BV and MTT differed significantly. Recipients with good outcomes showed persistent cirrhotic systemic hyperdynamics after LDLT, whereas recipients with poor outcomes presented with unstable cirrhotic systemic hyperdynamics and severely decreased K ICG. Systemic hyperdynamic disorders after LDLT impacted on portal venous flow but not hepatic arterial flow.
Conclusion: We conclude that subtle systemic hyperdynamics disorders impact on splanchnic circulation, and that an imbalance between CO and BV decreases portal venous flow, which results in critical outcomes.
Figures
References
-
- Hori T, Iida T, Yagi S, Taniguchi K, Yamamoto C, Mizuno S, Yamagiwa K, Isaji S, Uemoto S. K(ICG) value, a reliable real-time estimator of graft function, accurately predicts outcomes in adult living-donor liver transplantation. Liver Transpl. 2006;12:605–613. - PubMed
-
- Vorobioff J, Bredfeldt JE, Groszmann RJ. Increased blood flow through the portal system in cirrhotic rats. Gastroenterology. 1984;87:1120–1126. - PubMed
-
- Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J. Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology. 1998;8:1151–1157. - PubMed
-
- Yagi S, Iida T, Taniguchi K, Hori T, Hamada T, Fujii K, Mizuno S, Uemoto S. Impact of portal venous pressure on regeneration and graft damage after living-donor liver transplantation. Liver Transpl. 2005;11:68–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
