

Prognostic factors for survival in 676 consecutive patients with newly diagnosed primary glioblastoma
- PMID: 17993634
- PMCID: PMC2600841
- DOI: 10.1215/15228517-2007-038
Prognostic factors for survival in 676 consecutive patients with newly diagnosed primary glioblastoma
Abstract
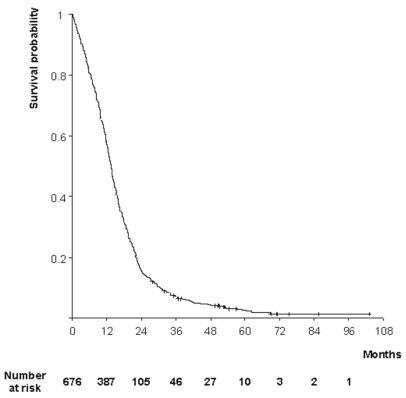
Reliable data on large cohorts of patients with glioblastoma are needed because such studies differ importantly from trials that have a strong bias toward the recruitment of younger patients with a higher performance status. We analyzed the outcome of 676 patients with histologically confirmed newly diagnosed glioblastoma who were treated consecutively at a single institution over a 7-year period (1997-2003) with follow-up to April 30, 2006. Survival probabilities were 57% at 1 year, 16% at 2 years, and 7% at 3 years. Progression-free survival was 15% at 1 year. Prolongation of survival was significantly associated with surgery in patients with a good performance status, whatever the patient's age, with an adjusted hazard ratio of 0.55 (p < 0.001) or a 45% relative decrease in the risk of death. Radiotherapy and chemotherapy improved survival, with adjusted hazard ratios of 0.61 (p = 0.001) and 0.89 (p = 0.04), respectively, regardless of age, performance status, or residual tumor volume. Recurrence occurred in 99% of patients throughout the follow-up. Reoperation was performed in one-fourth of these patients but was not effective, whether performed within 9 months (hazard ratio, 0.86; p = 0.256) or after 9 months (hazard ratio, 0.98; p = 0.860) of initial surgery, whereas second-line chemotherapy with procarbazine, lomustine, and vincristine (PCV) or with temozolomide improved survival (hazard ratio, 0.77; p = 0.008). Surgery followed by radiotherapy and chemotherapy should be considered in all patients with glioblastoma, and these treatments should not be withheld because of increasing age alone. The benefit of second surgery at recurrence is uncertain, and new trials are needed to assess its effectiveness. Chemotherapy with PCV or temozolomide seems to be a reasonable option at tumor recurrence.
Figures
References
-
- Ohgaki H, Dessen P, Jourde B, et al. Genetic pathways to glioblastoma: a population-based study. Cancer Res. 2004;64:6892 – 6899. - PubMed
-
- Stupp R, Pavlidis N, Jelic S for the ESMO Guidelines Task Force. ESMO minimum clinical recommendations for diagnosis, treatment and follow-up of malignant glioma. Ann Oncol. 2005;16(suppl 1):i64–i65. - PubMed
-
- Laperriere N, Zuraw L, Cairncross G Cancer Care Ontario Practice Guidelines Initiative Neuro-Oncology Disease Site Group. Radiotherapy for newly diagnosed malignant glioma in adults: a systematic review. Radiother Oncol. 2002;64:259 – 273. - PubMed
-
- Stuschke M, Thames HD. Hyperfractionated radiotherapy of human tumours: overview of the randomized clinical trials. Int J Radiat Oncol Biol Phys. 1997;37:259 – 267. - PubMed
-
- Behin A, Hoang-Xuan K, Carpentier AF, Delattre JY. Primary brain tumours in adults. Lancet. 2003;361:323 – 331. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
