

P2Y12 polymorphisms and antiplatelet effects of aspirin in patients with coronary artery disease
- PMID: 17995973
- PMCID: PMC2291388
- DOI: 10.1111/j.1365-2125.2007.03044.x
P2Y12 polymorphisms and antiplatelet effects of aspirin in patients with coronary artery disease
Abstract
What is already known about this subject: * Genetic polymorphisms of the P2Y(12) ADP receptor on platelets have been shown to contribute to variability in platelet aggregation in healthy humans. * P2Y(12) ADP receptor polymorphisms are more frequently present in patients with vascular disease than in healthy people. * The majority of patients with vascular disease receive acetylsalicylic acid as an anti-aggregatory agent, which has also been shown to induce a variable response; however, the role of P2Y(12) ADP receptor polymorphisms in the platelet response to acetylsalicylic acid in patients with vascular disease has not yet been studied.
What this study adds: * The present data show that the platelet response to acetylsalicylic acid is independent of the presence or absence of P2Y(12) ADP receptor polymorphisms in patients with stable coronary artery disease who have had their first myocardial infarction. * This is important, as studies in healthy humans had suggested that carriers of P2Y(12) ADP receptor polymorphisms may be at increased risk of experiencing cardiovascular events. * However, the observed variability of the platelet response to the cyclooxygenase inhibitor acetylsalicylic acid (in our study) and to the P2Y(12) ADP receptor blocker clopidogrel (in a study by Angiolillo et al) in patients with coronary artery disease is clearly not determined by common P2Y(12) ADP receptor polymorphisms.
Aims: Recently, two genetic polymorphisms of the platelet ADP receptor P2Y(12) (haplotypes H2 and 34T) have been implicated in increased platelet aggregation and atherothrombotic risk. It was suggested that these polymorphisms contribute to a diminished response to antiplatelet drugs. Therefore, we investigated the effects of these polymorphisms on platelet aggregation in aspirin-treated patients with coronary artery disease (CAD).
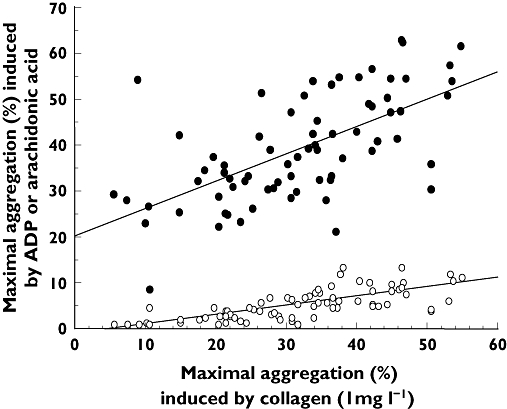
Methods: Platelet aggregation was studied in platelet-rich plasma from 124 patients with CAD treated with 100 mg aspirin day(-1). P2Y(12) ADP receptor polymorphisms were determined by PCR-RFLP. The 52G > T polymorphism was used as tag-SNP for the H2 haplotype. Aggregation was induced by 1 mg l(-1) collagen. In a subgroup (n = 72), a concentration-response curve to collagen (0.5-10 mg l(-1)), aggregation at 2 micromol l(-1) ADP and 1 mmol l(-1) arachidonic acid were determined.
Results: Whereas arachidonic acid-induced aggregation was inhibited in all patients, collagen and ADP-induced aggregation were highly variable. However, aggregation did not differ significantly between carriers and noncarriers of the 52T-allele (1 mg l(-1) collagen: 32.7% (21.9-38.6%) vs. 32.5% (21.2-41.6%); P = 0.77; ADP: 33.1% (29.9-40.9%) vs. 39.1% (31.5-49.7%); P = 0.34), respectively. EC(50) values were 1.26 mg l(-1) (0.79-2.02) and 1.54 mg l(-1) (0.98-2.4) collagen in noncarriers and carriers of the H2 haplotype, respectively (P = 0.56). Moreover, the 34 degrees C > T polymorphism did not significantly affect any of the aggregatory responses.
Conclusions: Low-dose aspirin inhibits platelet aggregation to the same extent in patients carrying or not carrying the P2Y(12) H2 haplotype and/or the 34T allele. Our data do not support the hypothesis that these polymorphisms contribute to an attenuated antiplatelet effect of aspirin.
Figures





References
-
- Hankey GJ, Eikelboom JW. Aspirin resistance. Lancet. 2006;367:606–17. - PubMed
-
- Wang TH, Bhatt DL, Topol EJ. Aspirin and clopidogrel resistance: an emerging clinical entity. Eur Heart J. 2006;27:647–54. - PubMed
-
- Daniel JL, Dangelmaier C, Jin J, Ashby B, Smith JB, Kunapuli SP. Molecular basis for ADP-induced platelet activation. I. Evidence for three distinct ADP receptors on human platelets. J Biol Chem. 1998;273:2024–9. - PubMed
-
- Hollopeter G, Jantzen HM, Vincent D, Li G, England L, Ramakrishnan V, Yang RB, Nurden P, Nurden A, Julius D, Conley PB. Identification of the platelet ADP receptor targeted by antithrombotic drugs. Nature. 2001;409:202–7. - PubMed
-
- Kauffenstein G, Bergmeier W, Eckly A, Ohlmann P, Leon C, Cazenave JP, Nieswandt B, Gachet C. The P2Y (12) receptor induces platelet aggregation through weak activation of the alpha (IIb) beta (3) integrin – a phosphoinositide 3-kinase-dependent mechanism. FEBS Lett. 2001;505:281–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
