

Precursors to pancreatic cancer
- PMID: 17996793
- PMCID: PMC2194627
- DOI: 10.1016/j.gtc.2007.08.012
Precursors to pancreatic cancer
Abstract
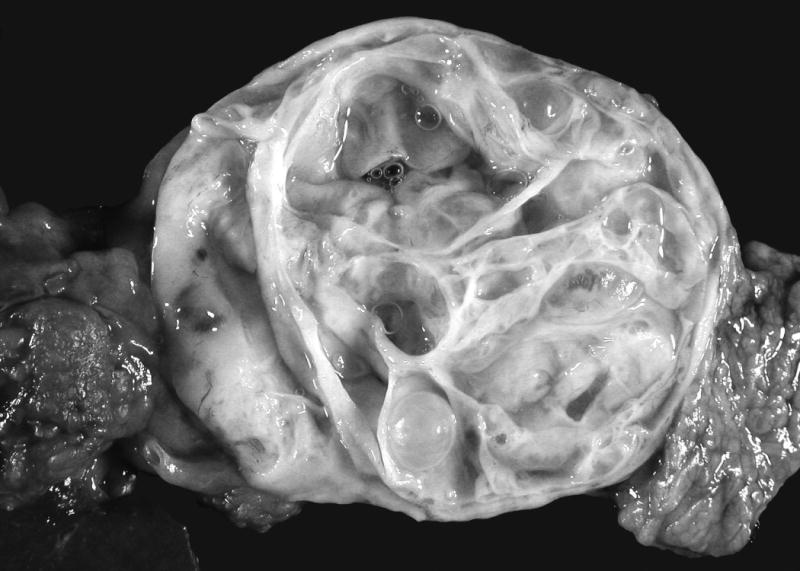
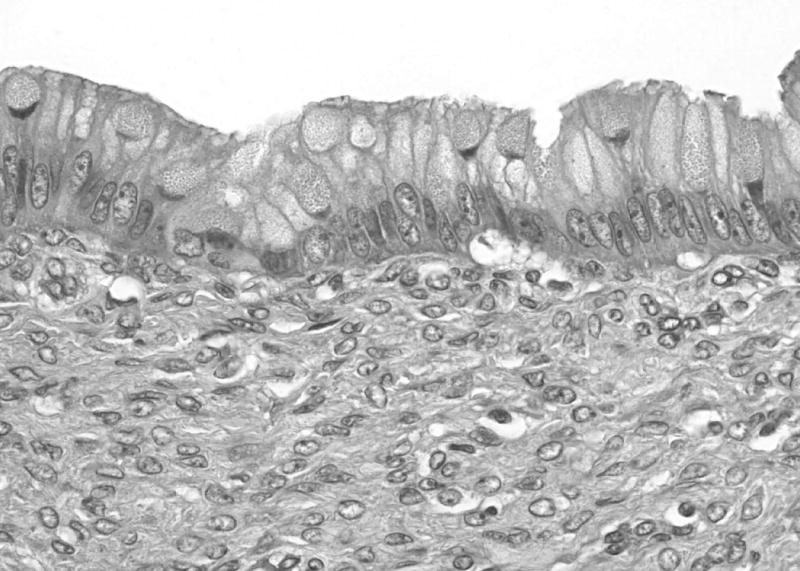
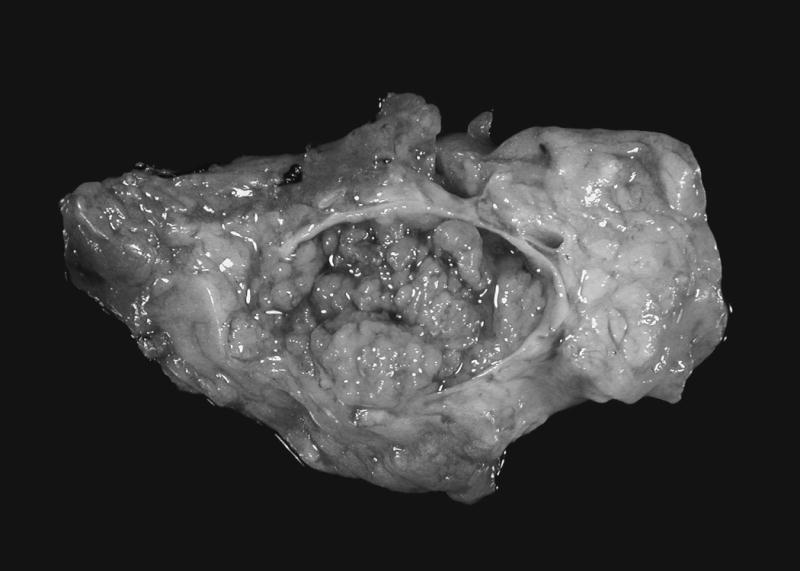
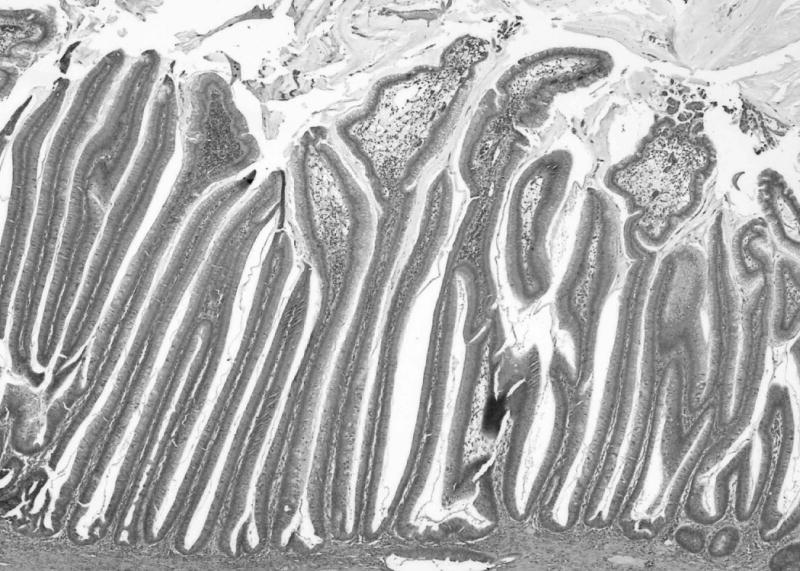
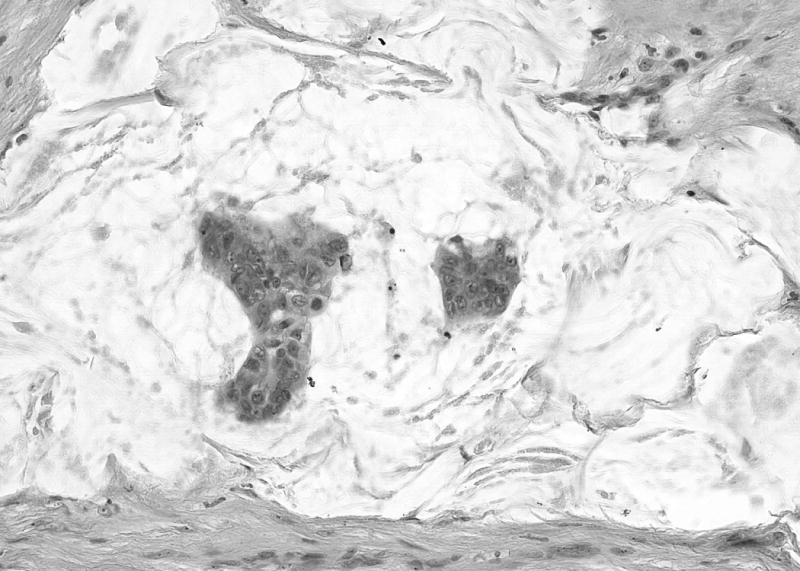
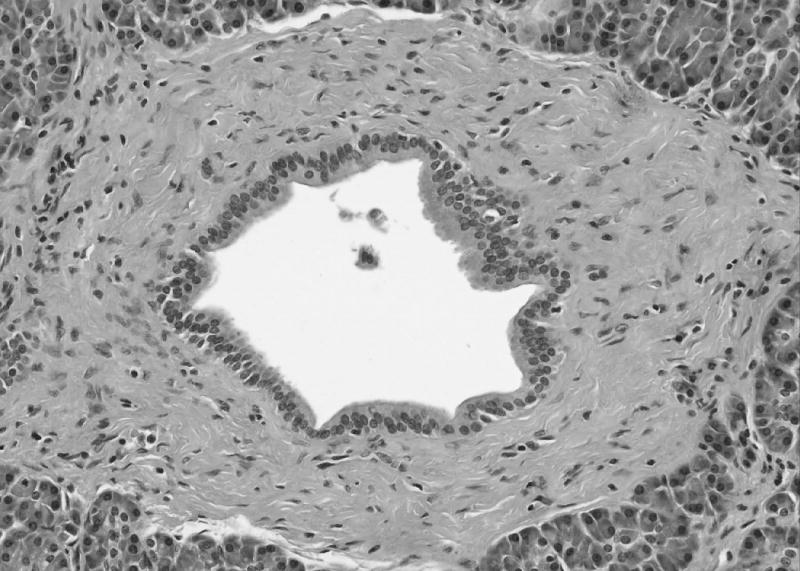
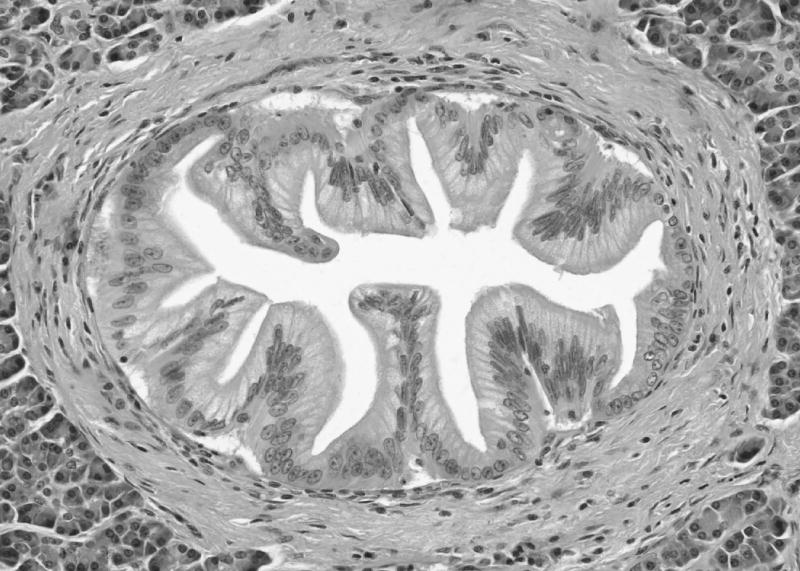
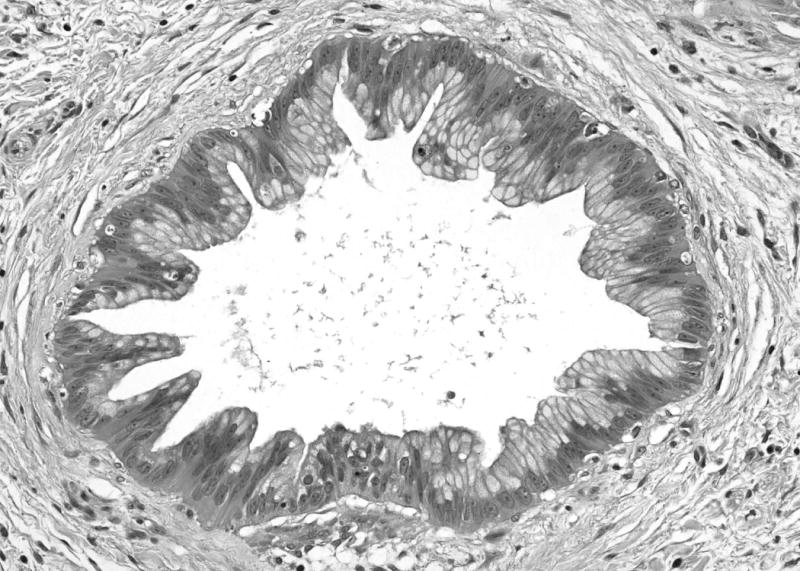
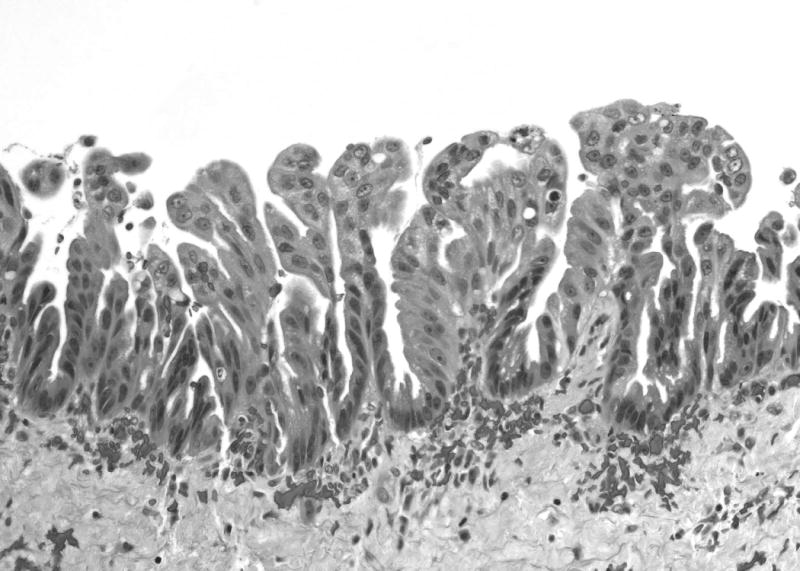
Infiltrating ductal adenocarcinoma of the pancreas is believed to arise from morphologically distinct noninvasive precursor lesions. These precursors include the intraductal papillary mucinous neoplasm, the mucinous cystic neoplasm, and pancreatic intraepithelial neoplasia. Intraductal papillary mucinous neoplasms are grossly visible mucin-producing epithelial neoplasms that arise in the main pancreatic duct or one of its branches. The cysts of mucinous cystic neoplasms do not communicate with the major pancreatic ducts, and these neoplasms are characterized by a distinct ovarian-type stroma. Pancreatic intraepithelial neoplasia is a microscopic lesion. This article focuses on the clinical significance of these three important precursor lesions, with emphasis on their clinical manifestations, detection, and treatment.
Figures
References
-
- American Cancer Society. Cancer. New York: New York, American Cancer Society; 2007. Cancer Facts & Figures 2007; pp. 1–52.
-
- Hruban RH, Pitman MB, Klimstra DS. Atlas of tumor pathology. Fascicle 6. Washington, DC: American Registry of Pathology and Armed Forces Institute of Pathology; 2007. Tumors of the pancreas. (Fourth).
-
- Hulst SPL. Zur kenntnis der Genese des Adenokarzinoms und Karzinoms des Pankreas. Virchows Arch (B) 1905;180:288–316.
-
- Hruban RH, Goggins M, Parsons JL, Kern SE. Progression model for pancreatic cancer. Clin Cancer Res. 2000;6:2969–2972. - PubMed
-
- Brat DJ, Lillemoe KD, Yeo CJ, Warfield PB, Hruban RH. Progression of pancreatic intraductal neoplasias to infiltrating adenocarcinoma of the pancreas. Am J Surg Pathol. 1998;22(2):163–169. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
