

Sleep-specific mechanisms underlying posttraumatic stress disorder: integrative review and neurobiological hypotheses
- PMID: 17997114
- PMCID: PMC2490669
- DOI: 10.1016/j.smrv.2007.09.003
Sleep-specific mechanisms underlying posttraumatic stress disorder: integrative review and neurobiological hypotheses
Abstract
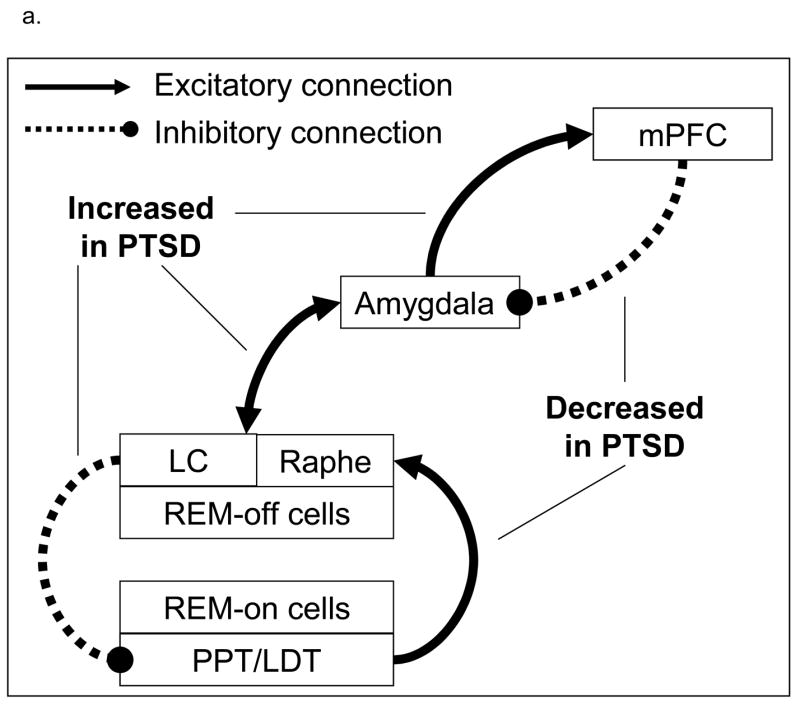
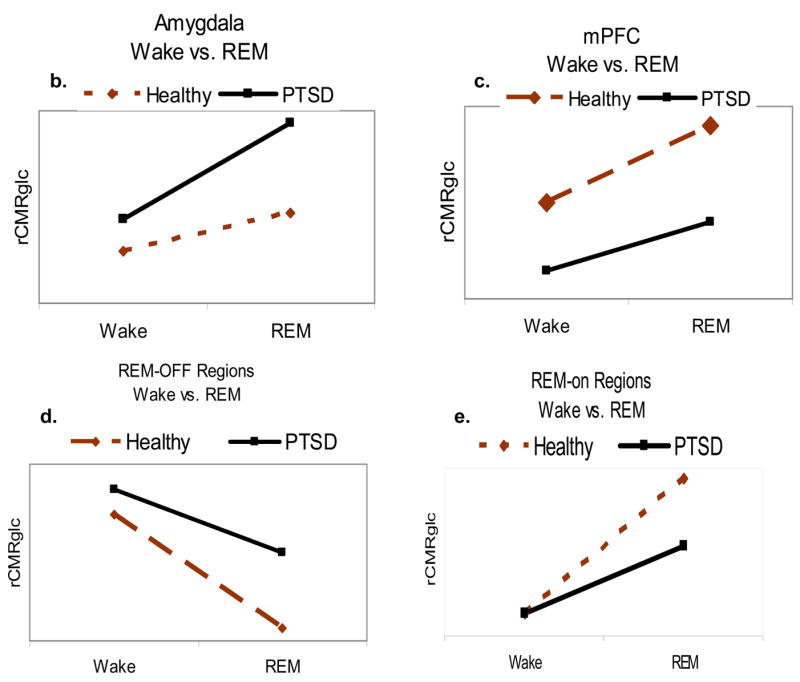
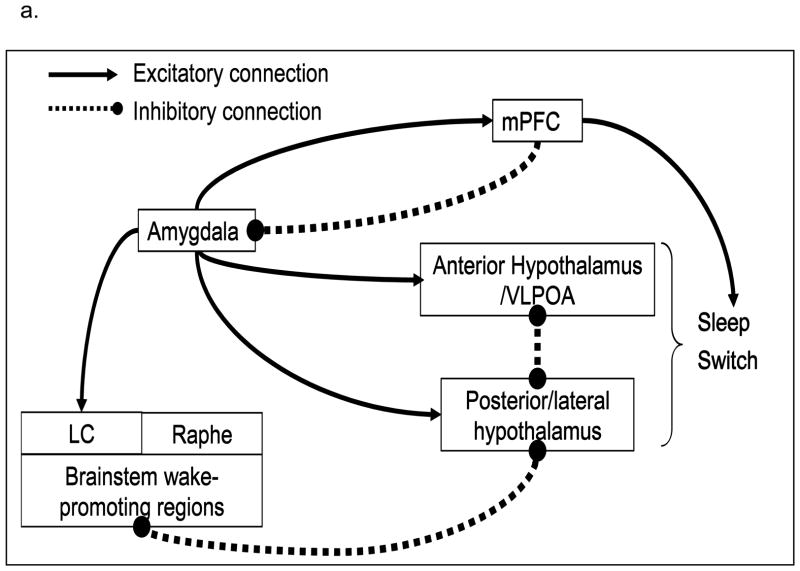
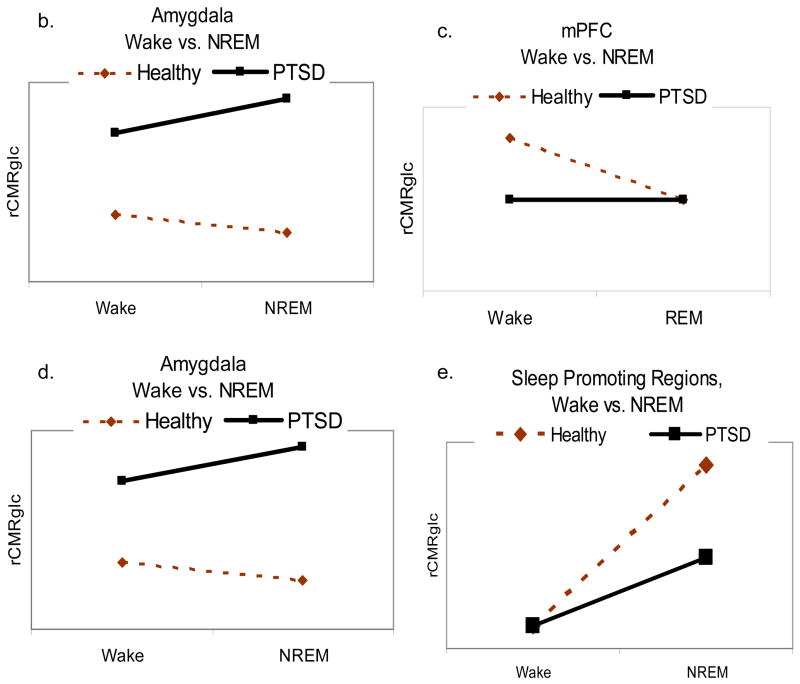
Posttraumatic stress disorder (PTSD) is a prevalent disorder that is associated with poor clinical and health outcomes, and considerable health care utilization and costs. Recent estimates suggest that 5-20% of military personnel who serve in current conflicts in Iraq and Afghanistan meet diagnostic criteria for PTSD. Clinically, sleep disturbances are core features of PTSD that are often resistant to first-line treatments, independently contribute to poor daytime functioning, and often require sleep-focused treatments. Physiologically, these observations suggest that PTSD is partially mediated by sleep disruption and its neurobiological correlates that are not adequately addressed by first-line treatments. However, polysomnographic studies have provided limited insights into the neurobiological underpinnings of PTSD during sleep. There is an urgent need to apply state-of-the-science sleep measurement methods to bridge the apparent gap between the clinical significance of sleep disturbances in PTSD and the limited understanding of their neurobiological underpinnings. Here, we propose an integrative review of findings derived from neurobiological models of fear conditioning and fear extinction, PTSD, and sleep-wake regulation, suggesting that the amygdala and medial prefrontal cortex can directly contribute to sleep disturbances in PTSD. Testable hypotheses regarding the neurobiological underpinnings of PTSD across the sleep-wake cycle are offered.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 4. Washington, DC: American Psychiatric Association; 1994.
-
- Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, Andreski P. Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry. 1998;55(7):626–632. - PubMed
-
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52(12):1048–1060. - PubMed
-
- Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, Best CL. Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women. J Consult Clin Psychol. 1993;61(6):984–991. - PubMed
-
- Weiss DS, Marmar CR, Schlenger WE, Fairbank JA, Jordan BK, Hough RL, et al. The prevalence of lifetime and partial post-traumatic stress disorder in Vietnam theater veterans. J Trauma Stress. 1992;5:365–376.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
