

Obesity and mortality in men with locally advanced prostate cancer: analysis of RTOG 85-31
- PMID: 17999404
- PMCID: PMC3047389
- DOI: 10.1002/cncr.23093
Obesity and mortality in men with locally advanced prostate cancer: analysis of RTOG 85-31
Abstract
Background: Greater body mass index (BMI) is associated with shorter time to prostate-specific antigen (PSA) failure following radical prostatectomy and radiation therapy (RT). Whether BMI is associated with prostate cancer-specific mortality (PCSM) was investigated in a large randomized trial of men treated with RT and androgen deprivation therapy (ADT) for locally advanced prostate cancer.
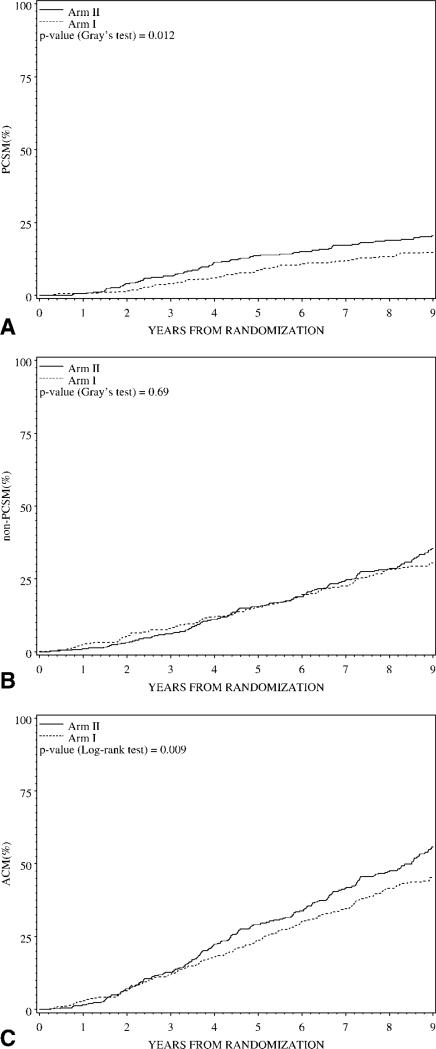
Methods: Between 1987 and 1992, 945 eligible men with locally advanced prostate cancer were enrolled in a phase 3 trial (RTOG 85-31) and randomized to RT and immediate goserelin or RT alone followed by goserelin at recurrence. Height and weight data were available at baseline for 788 (83%) subjects. Cox regression analyses were performed to evaluate the relations between BMI and all-cause mortality, PCSM, and nonprostate cancer mortality. Covariates included age, race, treatment arm, history of prostatectomy, nodal involvement, Gleason score, clinical stage, and BMI.
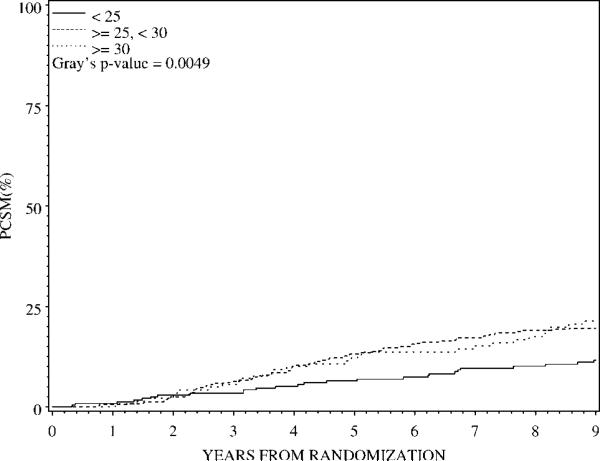
Results: The 5-year PCSM rate for men with BMI <25 kg/m(2) was 6.5%, compared with 13.1% and 12.2% in men with BMI > or =25 to <30 and BMI > or =30, respectively (Gray's P = .005). In multivariate analyses, greater BMI was significantly associated with higher PCSM (for BMI > or =25 to <30, hazard ratio [HR] 1.52, 95% confidence interval [CI], 1.02-2.27, P = .04; for BMI > or =30, HR 1.64, 95% CI, 1.01-2.66, P = .04). BMI was not associated with nonprostate cancer or all-cause mortality.
Conclusions: Greater baseline BMI is independently associated with higher PCSM in men with locally advanced prostate cancer. Further studies are warranted to evaluate the mechanism(s) for increased cancer-specific mortality and to assess whether weight loss after prostate cancer diagnosis alters disease course.
2007 American Cancer Society
Figures
References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–1555. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861–1867. - PubMed
-
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–1638. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
