

Neuroimaging findings in macrocephaly-capillary malformation: a longitudinal study of 17 patients
- PMID: 18000912
- PMCID: PMC6816457
- DOI: 10.1002/ajmg.a.32040
Neuroimaging findings in macrocephaly-capillary malformation: a longitudinal study of 17 patients
Abstract
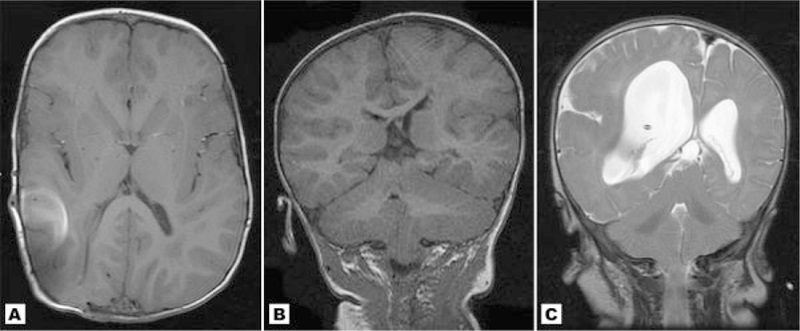
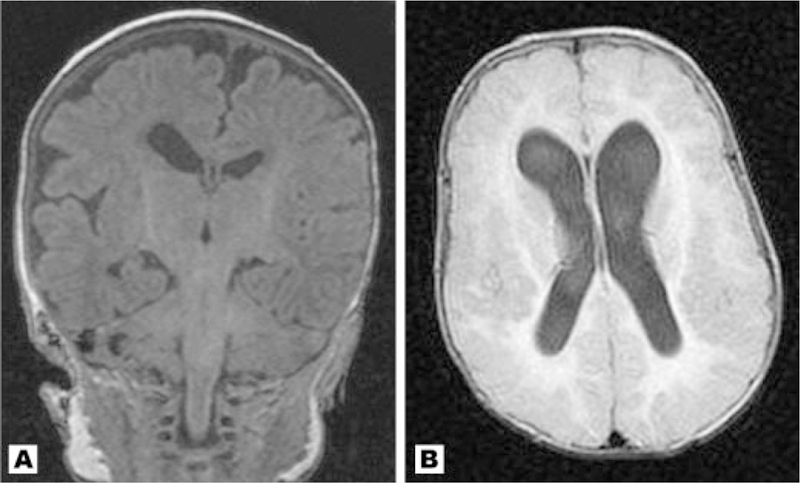
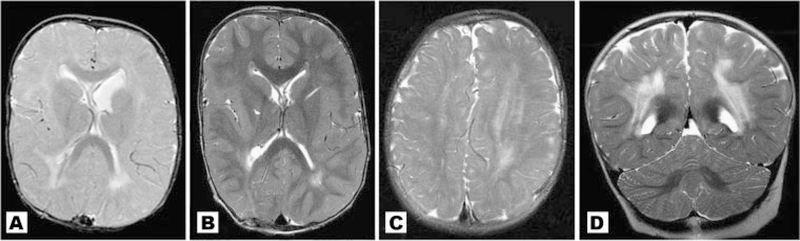
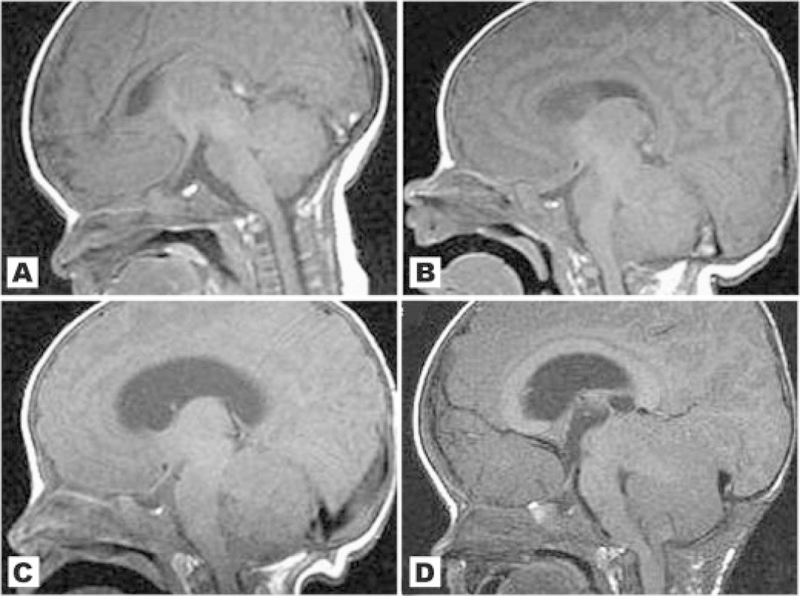
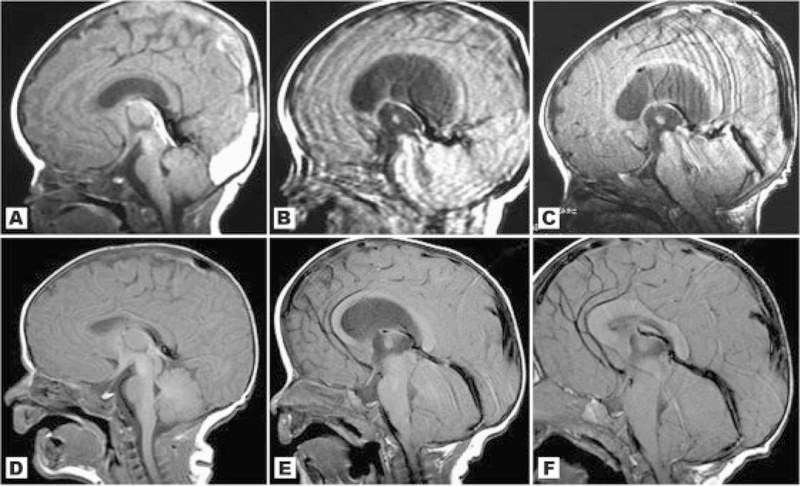
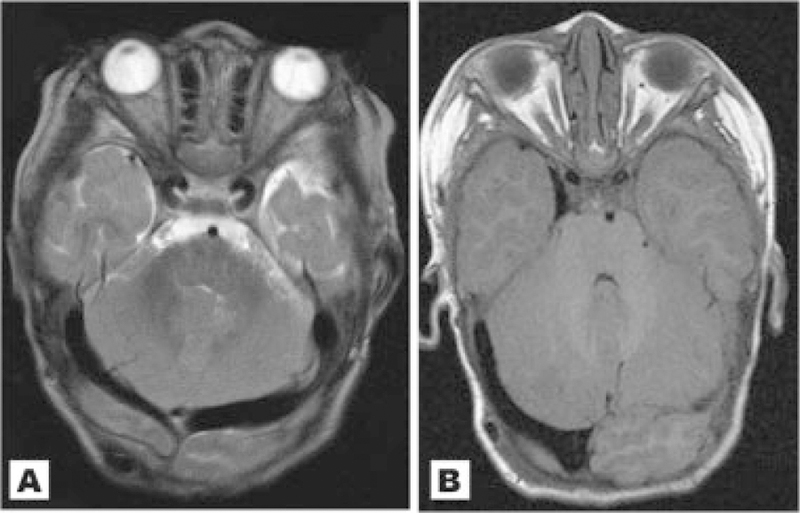
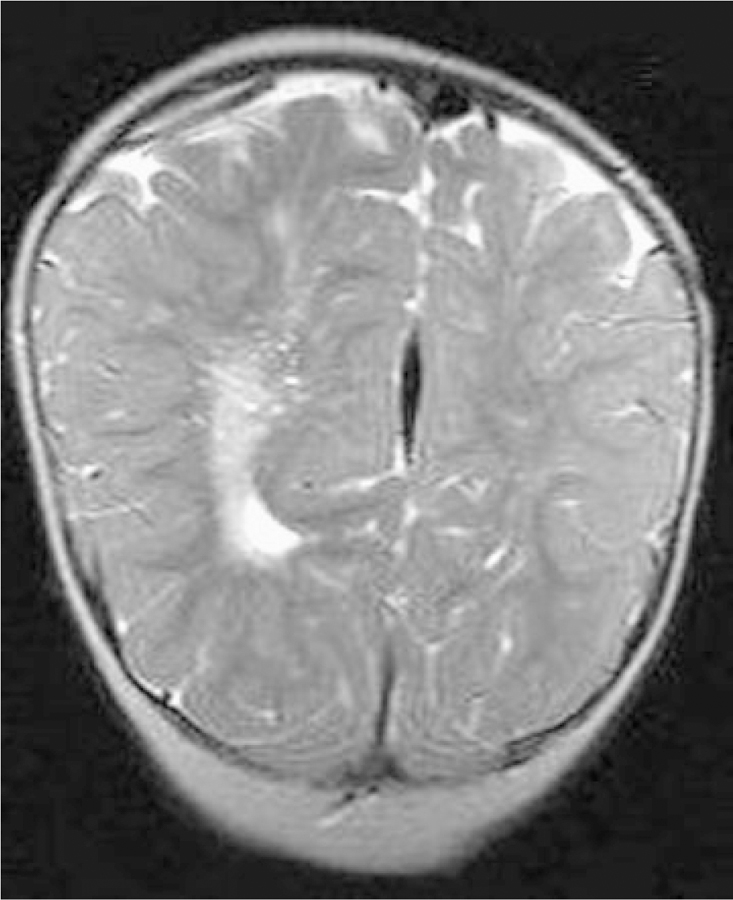
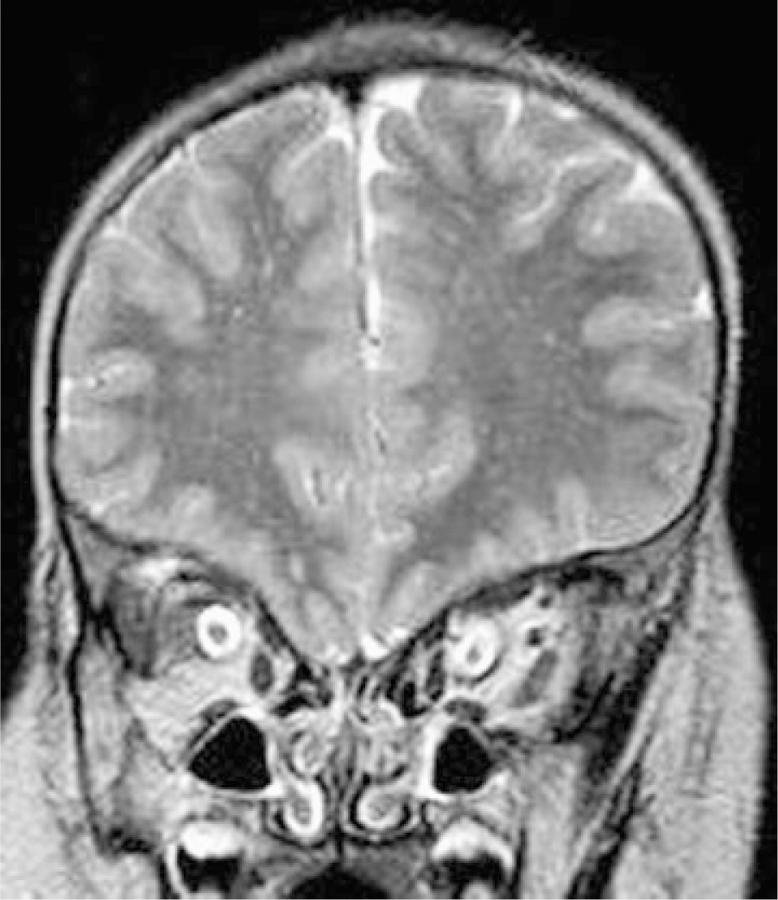
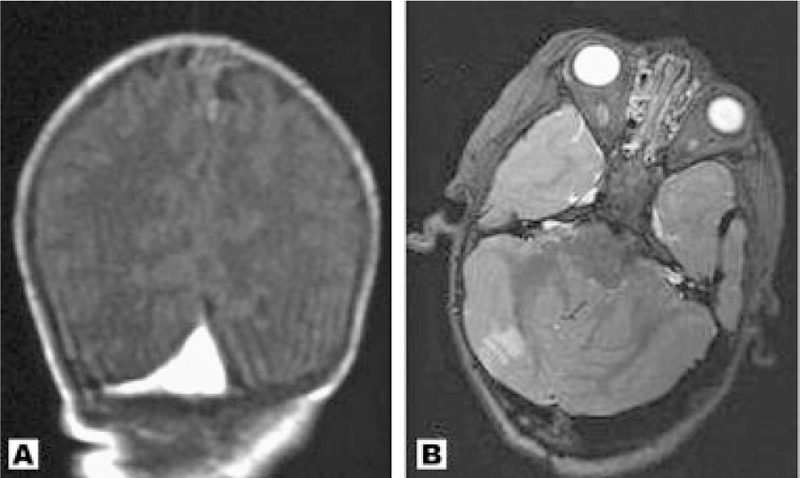
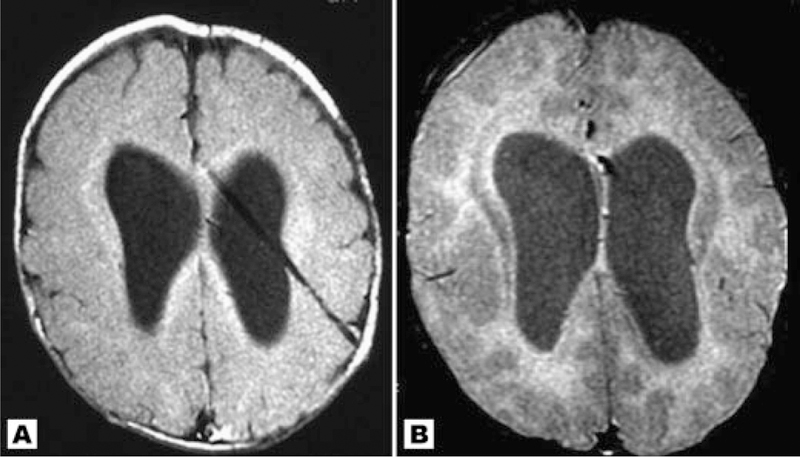
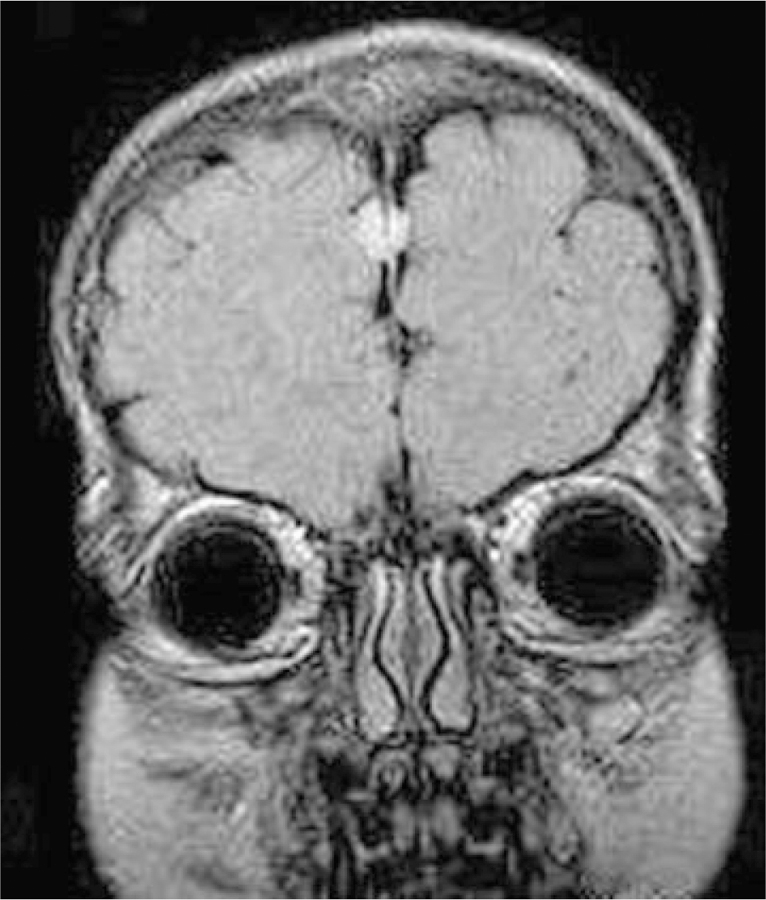
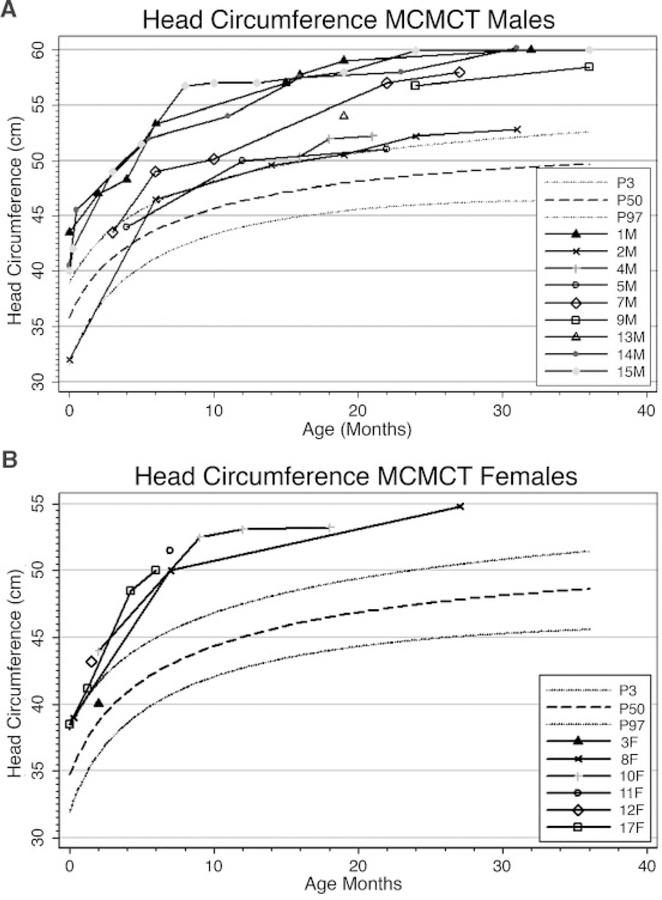
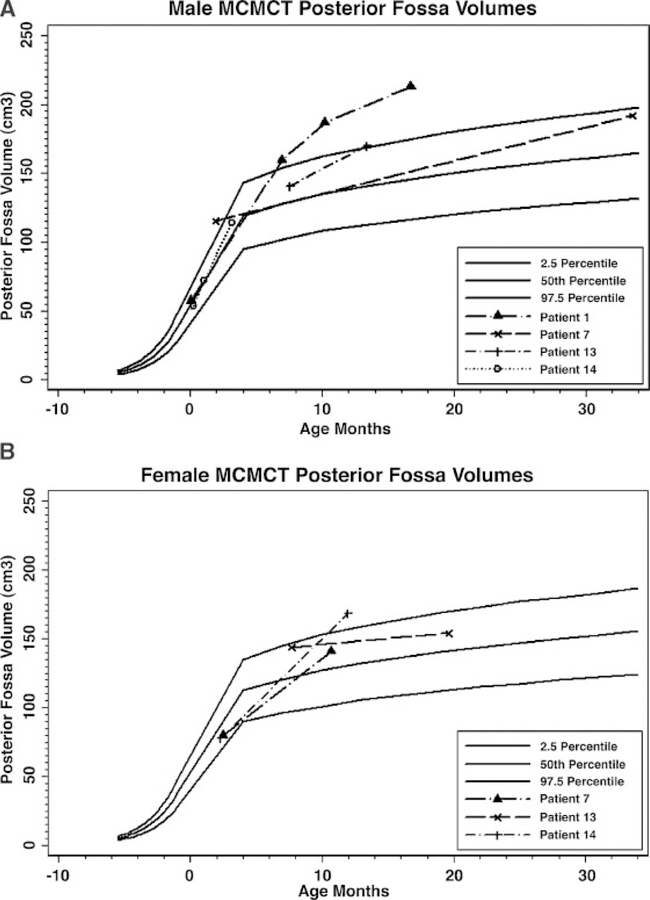
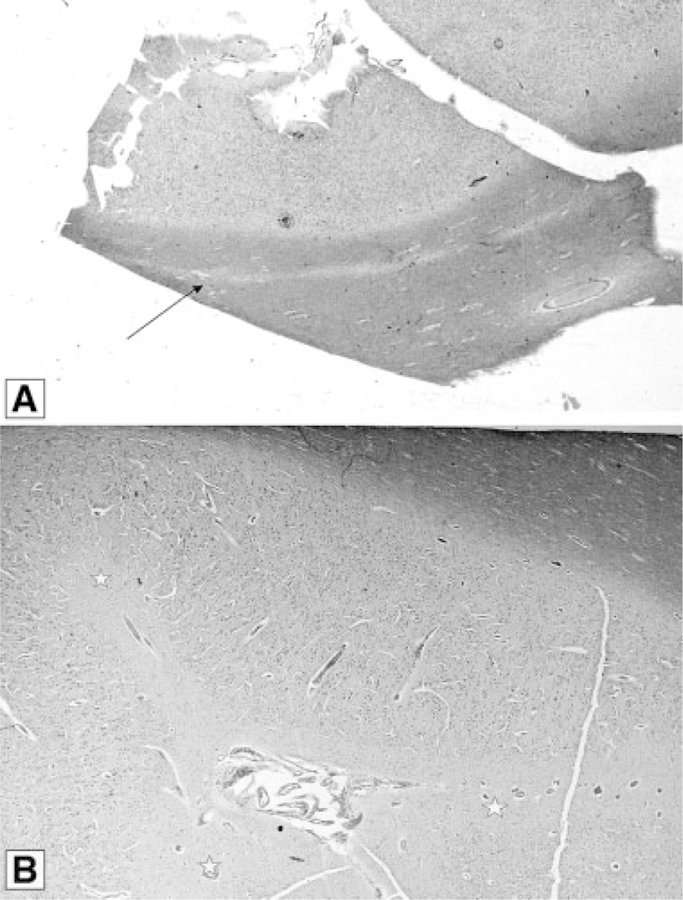
Here, we report the neuroimaging findings and neurological changes in 17 unpublished patients with Macrocephaly-Capillary Malformation (M-CM). This syndrome has been traditionally known as Macrocephaly-Cutis Marmorata Telangiectatica Congenita (M-CMTC), but we explain why M-CM is a more accurate term for this overgrowth syndrome. We analyzed the 17 patients with available brain MRI or CT scans and compared their findings with features identified by a comprehensive review of published cases. White matter irregularities with increased signal on T2-weighted images were commonly observed findings. A distinctive feature in more than half the patients was cerebellar tonsillar herniation associated with rapid brain growth and progressive crowding of the posterior fossa during infancy. In four such cases, we confirmed that the tonsillar herniation was an acquired event. Concurrently, with the development of these findings, ventriculomegaly (frequently obstructive) and dilated dural venous sinuses were observed in conjunction with prominent Virchow-Robin spaces in many of those in whom cerebellar tonsil herniation had developed. We postulate that this constellation of unusual features suggests a dynamic process of mechanical compromise in the posterior fossa, perhaps initiated by a rapidly growing cerebellum, which leads to congestion of the venous drainage with subsequently compromised cerebrospinal fluid reabsorption, all of which increases the posterior fossa pressure and leads to acquired tonsillar herniation. We make a distinction between congenital Chiari I malformation and acquired cerebellar tonsil herniation in this syndrome. We also observed numerous examples of abnormal cortical morphogenesis, including focal cortical dysplasia, polymicrogyria which primarily involved the perisylvian and insular regions, and cerebral and/or cerebellar asymmetric overgrowth. Other findings included a high frequency of cavum septum pellucidum or vergae, thickened corpus callosum, prominent optic nerve sheaths and a single case of venous sinus thrombosis. One patient was found to have a frontal perifalcine mass resembling a meningioma at age 5 years. This is the second apparent occurrence of this specific tumor in M-CM.
(c) 2007 Wiley-Liss, Inc.
Figures

References
-
- Abeloff MD, Armitage JO, Niederhuber JE, Kastan MB, Gillies McKenna W. 2004. Clinical oncology. 3rd edition. New York: Churchill Livingstone.
-
- Ackar N, Adapinar B, Dinleyici C, Durak B, Ozkan IR. 2004. A case of macrocephaly-cutis marmorata telangiectatica congenita and review of neuroradiologic features. Ann Genet 47:261–265. - PubMed
-
- AnalyzeDirect. Analyze Versions 6.0 and 7.0.
-
- Artigas J, Poo P, Rovira A, Cardo E. 1999. Macrocephaly and dilated Virchow-Robin spaces in childhood. Pediatr Radiol 29:188–190. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
