

Arrhythmogenic right ventricular cardiomyopathy/dysplasia
- PMID: 18001465
- PMCID: PMC2222049
- DOI: 10.1186/1750-1172-2-45
Arrhythmogenic right ventricular cardiomyopathy/dysplasia
Abstract
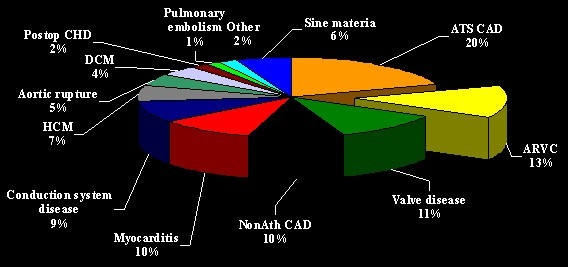
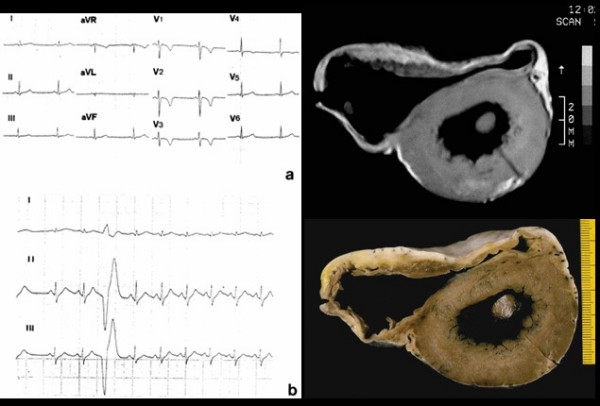
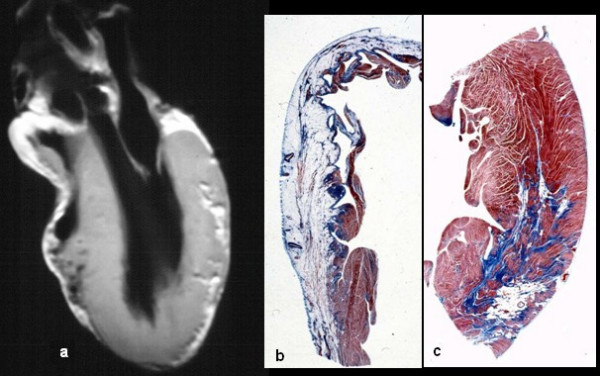
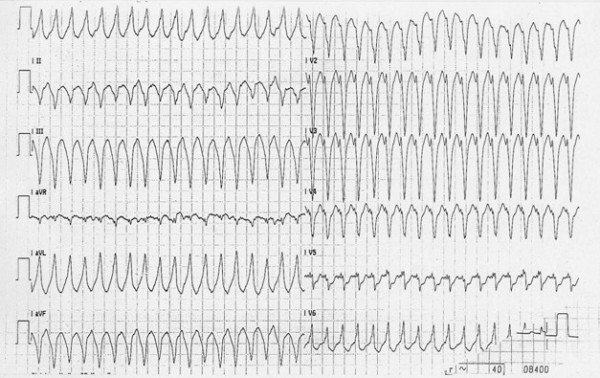
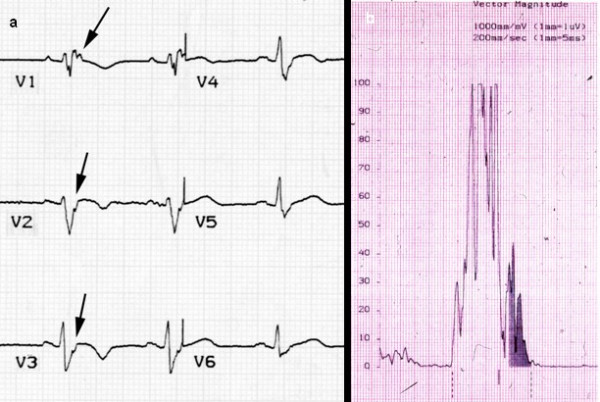
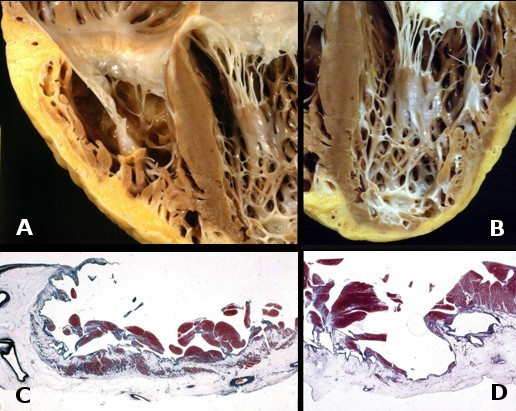
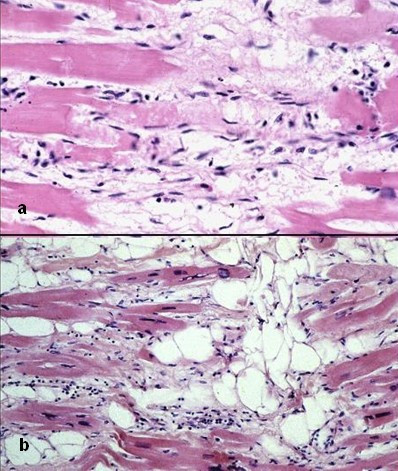
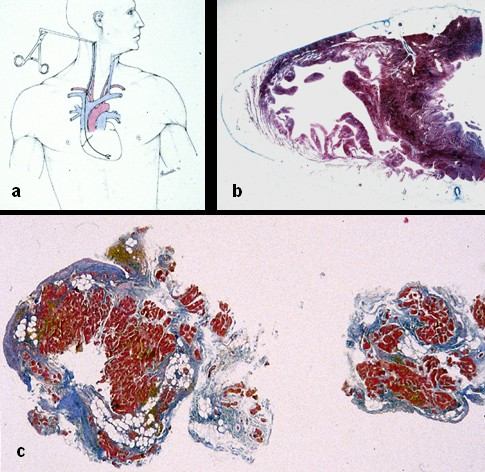
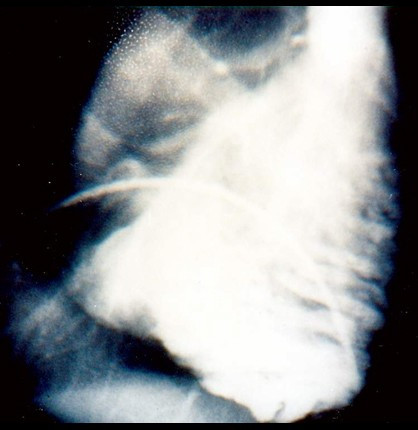
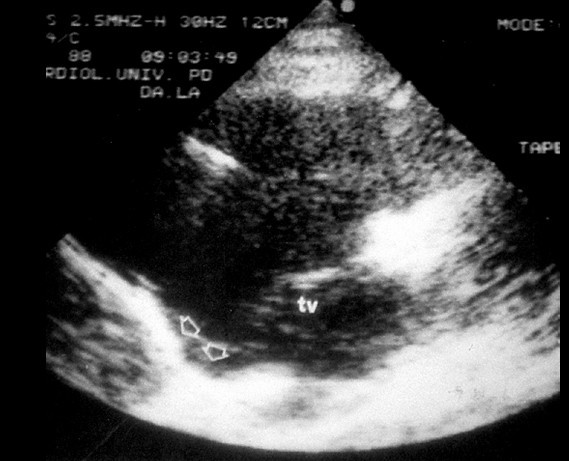
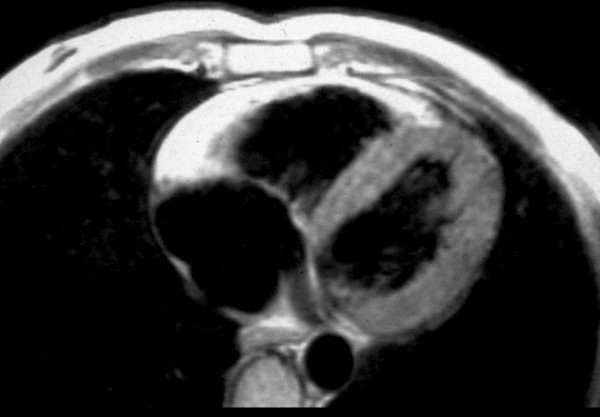
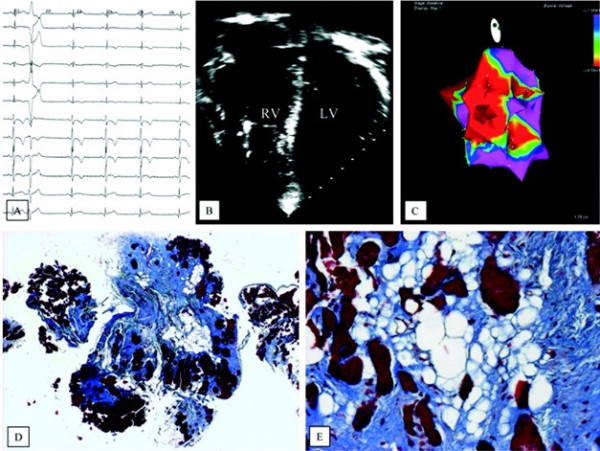
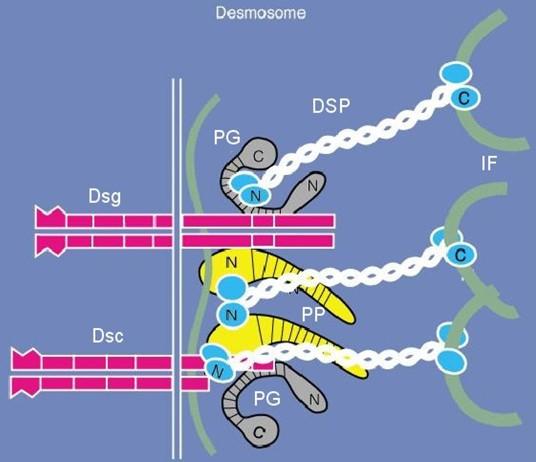
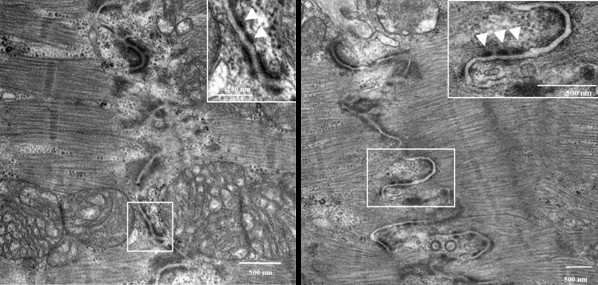
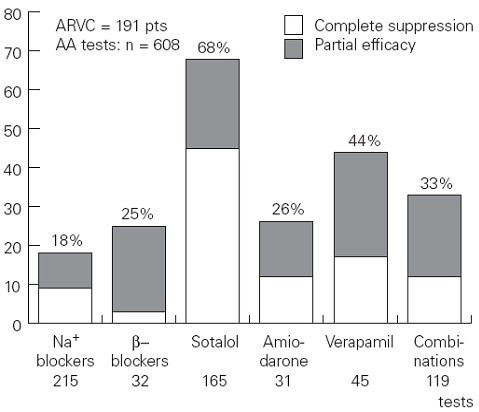
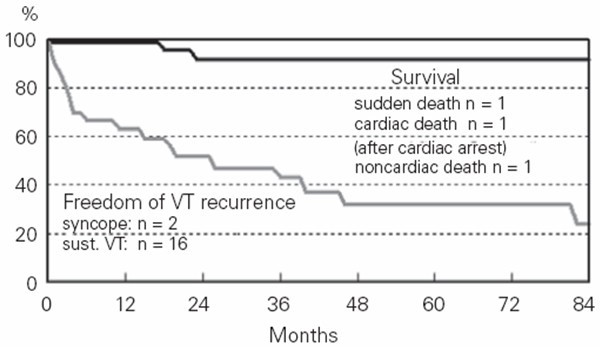
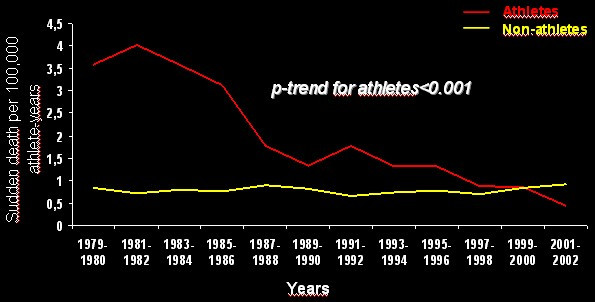
Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) is a heart muscle disease clinically characterized by life-threatening ventricular arrhythmias. Its prevalence has been estimated to vary from 1:2,500 to 1:5,000. ARVC/D is a major cause of sudden death in the young and athletes. The pathology consists of a genetically determined dystrophy of the right ventricular myocardium with fibro-fatty replacement to such an extent that it leads to right ventricular aneurysms. The clinical picture may include: a subclinical phase without symptoms and with ventricular fibrillation being the first presentation; an electrical disorder with palpitations and syncope, due to tachyarrhythmias of right ventricular origin; right ventricular or biventricular pump failure, so severe as to require transplantation. The causative genes encode proteins of mechanical cell junctions (plakoglobin, plakophilin, desmoglein, desmocollin, desmoplakin) and account for intercalated disk remodeling. Familiar occurrence with an autosomal dominant pattern of inheritance and variable penetrance has been proven. Recessive variants associated with palmoplantar keratoderma and woolly hair have been also reported. Clinical diagnosis may be achieved by demonstrating functional and structural alterations of the right ventricle, depolarization and repolarization abnormalities, arrhythmias with the left bundle branch block morphology and fibro-fatty replacement through endomyocardial biopsy. Two dimensional echo, angiography and magnetic resonance are the imaging tools for visualizing structural-functional abnormalities. Electroanatomic mapping is able to detect areas of low voltage corresponding to myocardial atrophy with fibro-fatty replacement. The main differential diagnoses are idiopathic right ventricular outflow tract tachycardia, myocarditis, dialted cardiomyopathy and sarcoidosis. Only palliative therapy is available and consists of antiarrhythmic drugs, catheter ablation and implantable cardioverter defibrillator. Young age, family history of juvenile sudden death, QRS dispersion > or = 40 ms, T-wave inversion, left ventricular involvement, ventricular tachycardia, syncope and previous cardiac arrest are the major risk factors for adverse prognosis. Preparticipation screening for sport eligibility has been proven to be effective in detecting asymptomatic patients and sport disqualification has been life-saving, substantially declining sudden death in young athletes.
Figures
References
-
- Marcus F, Fontaine G, Guirdaudon G, Frank R, Laurenceau JL, Malergue C, Grosgogeat Y. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–398. - PubMed
-
- Nava A, Thiene G, Canciani B, Scognamiglio R, Daliento L, Buja G, Martini B, Stritoni P, Fasoli G. Familial occurrence of right ventricular dysplasia: a study involving nine families. J Am Coll Cardiol. 1988;12:1222–1228. - PubMed
-
- Thiene G, Nava A, Corrado D, Rossi L, Pennelli N. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med. 1988;318:129–133. - PubMed
-
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M. Arrhythmogenic right ventricular cardiomyopathy: dysplasia, dystrophy or myocarditis ? Circulation. 1996;94:983–991. - PubMed
-
- McKenna WJ, Thiene G, Nava A, Fontaliran F, Blomstrom-Lundqvist C, Fontaine G, Camerini F. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br Heart J. 1994;71:215–218. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
