

Impact of attention-deficit/hyperactivity disorder (ADHD) on prescription dug spending for children and adolescents: increasing relevance of health economic evidence
- PMID: 18005403
- PMCID: PMC2216002
- DOI: 10.1186/1753-2000-1-13
Impact of attention-deficit/hyperactivity disorder (ADHD) on prescription dug spending for children and adolescents: increasing relevance of health economic evidence
Abstract
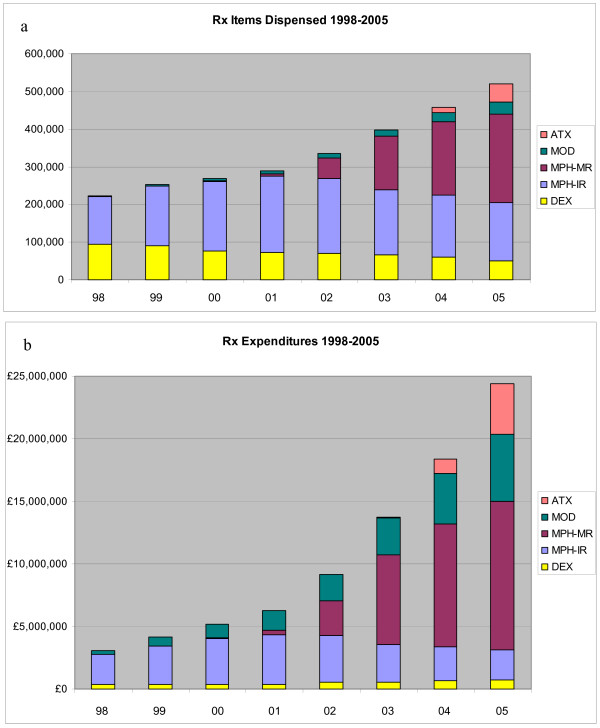
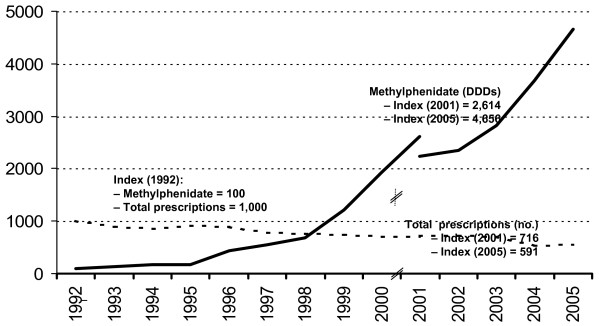
Background: During the last decade, pharmaceutical spending for patients with attention-deficit-hyperactivity disorder (ADHD) has been escalating internationally.
Objectives: First, to estimate future trends of ADHD-related drug expenditures from the perspectives of the statutory health insurance (SHI; Gesetzliche Krankenversicherung, GKV) in Germany and the National Health Service (NHS) in England, respectively, for children and adolescents age 6 to 18 years. Second, to evaluate the budgetary impact on individual prescribers (child and adolescent psychiatrists and pediatricians treating patients with ADHD) in Germany.
Methods: A model was developed to predict plausible scenarios of future pharmaceutical expenditures for treatment of ADHD. Model inputs were derived from demographic and epidemiological data, a literature review of past spending trends, and an analysis of new pharmaceutical products in development for ADHD. Only products in clinical development phase III or later were considered. Uncertainty was addressed by way of scenario analysis. For each jurisdiction, five scenarios used different assumptions of future diagnosis prevalence, treatment prevalence, rates of adoption and unit costs of novel drugs, and treatment intensity.
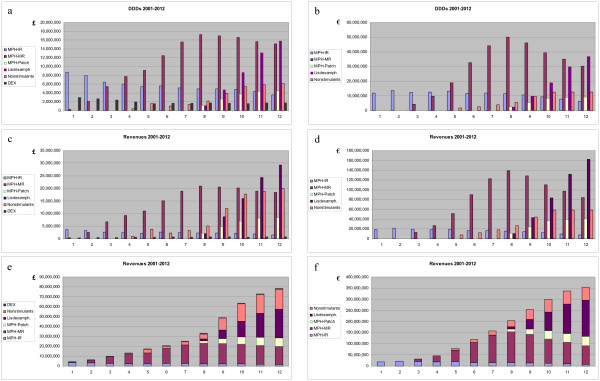
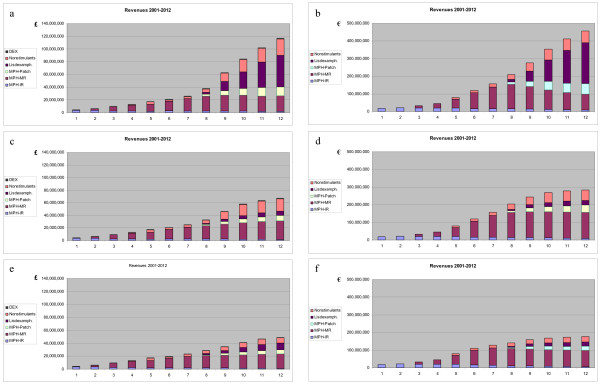
Results: Annual ADHD pharmacotherapy expenditures for children and adolescents will further increase and may exceed euro 310 m (D; E: 78 m) in 2012 (2002: approximately euro 21.8 m; approximately 7.0 m). During this period, overall drug spending by individual physicians may increase 2.3- to 9.5-fold, resulting from the multiplicative effects of four variables: increased number of diagnosed cases, growing acceptance and intensity of pharmacotherapy, and higher unit costs of novel medications.
Discussion: Even for an extreme low case scenario, a more than six-fold increase of pharmaceutical spending for children and adolescents is predicted over the decade from 2002 to 2012, from the perspectives of both the NHS in England and the GKV in Germany. This budgetary impact projection represents a partial analysis only because other expenditures are likely to rise as well, for instance those associated with physician services, including diagnosis and psychosocial treatment. Further to this, by definition budgetary impact analyses have little to nothing to say about clinical appropriateness and about value of money.
Conclusion: Providers of care for children and adolescents with ADHD should anticipate serious challenges related to the cost-effectiveness of interventions.
Figures

Similar articles
-
[The health economics of attention deficit hyperactivity disorder in Germany. Part 1: Health care utilization and cost of illness].Nervenarzt. 2010 Mar;81(3):289-300. doi: 10.1007/s00115-009-2888-9. Nervenarzt. 2010. PMID: 20232510 Review. German.
-
Impact of 3-tier formularies on drug treatment of attention-deficit/hyperactivity disorder in children.Arch Gen Psychiatry. 2005 Apr;62(4):435-41. doi: 10.1001/archpsyc.62.4.435. Arch Gen Psychiatry. 2005. PMID: 15809411 Free PMC article.
-
Treatment costs of attention deficit hyperactivity disorder in Germany.Eur J Health Econ. 2013 Dec;14(6):939-45. doi: 10.1007/s10198-012-0440-5. Epub 2012 Nov 21. Eur J Health Econ. 2013. PMID: 23179162
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
-
Economic Burden of Attention-Deficit/Hyperactivity Disorder among Pediatric Patients in the United States.Value Health. 2017 Apr;20(4):602-609. doi: 10.1016/j.jval.2017.01.007. Value Health. 2017. PMID: 28408002
Cited by
-
Prevalence of attention-deficit hyperactivity disorder (ADHD): systematic review and meta-analysis.Eur Psychiatry. 2024 Oct 9;67(1):e68. doi: 10.1192/j.eurpsy.2024.1786. Eur Psychiatry. 2024. PMID: 39381949 Free PMC article.
-
The NICE ADHD health technology assessment: a review and critique.Child Adolesc Psychiatry Ment Health. 2008 Jan 15;2(1):1. doi: 10.1186/1753-2000-2-1. Child Adolesc Psychiatry Ment Health. 2008. PMID: 18197978 Free PMC article.
-
[The health economics of attention deficit hyperactivity disorder in Germany. Part 1: Health care utilization and cost of illness].Nervenarzt. 2010 Mar;81(3):289-300. doi: 10.1007/s00115-009-2888-9. Nervenarzt. 2010. PMID: 20232510 Review. German.
-
Protocol investigating the clinical utility of an objective measure of activity and attention (QbTest) on diagnostic and treatment decision-making in children and young people with ADHD-'Assessing QbTest Utility in ADHD' (AQUA): a randomised controlled trial.BMJ Open. 2014 Dec 1;4(12):e006838. doi: 10.1136/bmjopen-2014-006838. BMJ Open. 2014. PMID: 25448628 Free PMC article. Clinical Trial.
-
Protocol investigating the clinical utility of an objective measure of attention, impulsivity and activity (QbTest) for optimising medication management in children and young people with ADHD 'QbTest Utility for Optimising Treatment in ADHD' (QUOTA): a feasibility randomised controlled trial.BMJ Open. 2018 Feb 15;8(2):e021104. doi: 10.1136/bmjopen-2017-021104. BMJ Open. 2018. PMID: 29453304 Free PMC article. Clinical Trial.
References
-
- Zito JM, Safer DJ, dosReis S, Magder LS, Gardner JF, Zarin DA. Psychotherapeutic medication patterns for youths with attention-deficit hyperactivity disorder. Archives of Pediatrics & Adolescent Medicine. 1999;153:1257–1263. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
