

Meta-analysis of the relation between European and American smokeless tobacco and oral cancer
- PMID: 18005437
- PMCID: PMC2225413
- DOI: 10.1186/1471-2458-7-334
Meta-analysis of the relation between European and American smokeless tobacco and oral cancer
Abstract
Background: Smokeless tobacco is often referred to as a major contributor to oral cancer. In some regions, especially Southeast Asia, the risk is difficult to quantify due to the variety of products, compositions (including non-tobacco ingredients) and usage practices involved. In Western populations, the evidence of an increased risk in smokeless tobacco users seems unclear, previous reviews having reached somewhat differing conclusions. We report a detailed quantitative review of the evidence in American and European smokeless tobacco users, and compare our findings with previous reviews and meta-analyses.
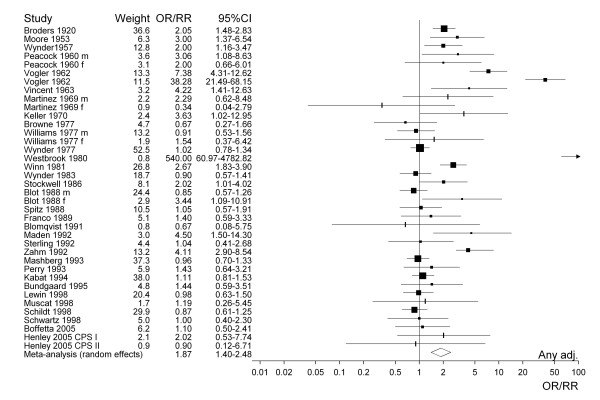
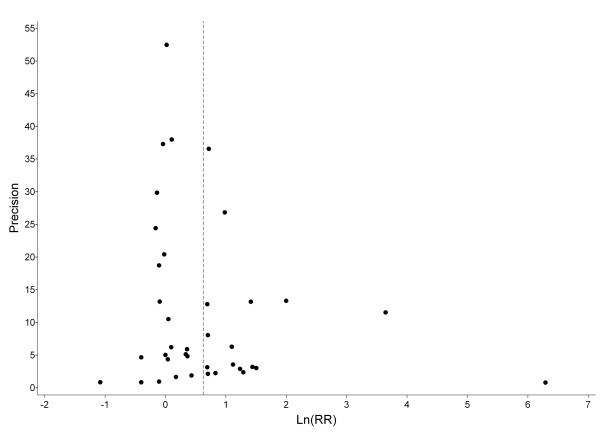
Methods: Following literature review a meta-analysis was conducted of 32 epidemiological studies published between 1920 and 2005 including tests for homogeneity and publication bias.
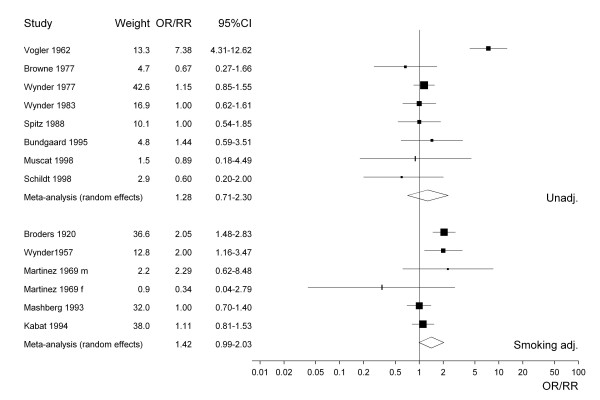
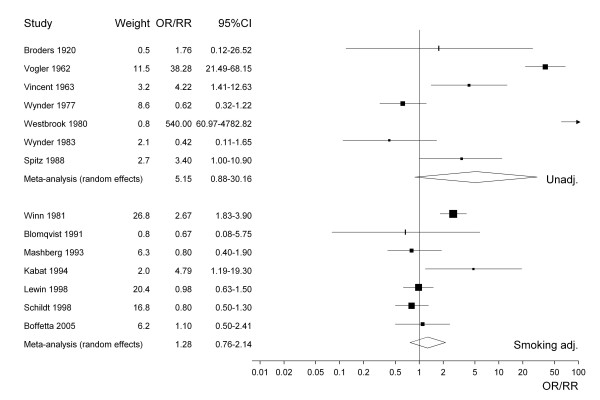
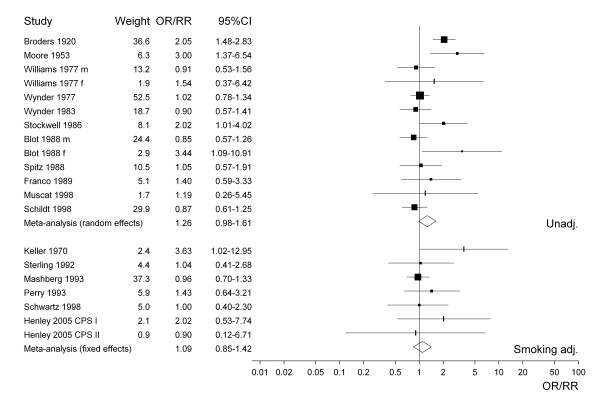
Results: Based on 38 heterogeneous study-specific estimates of the odds ratio or relative risk for smokeless tobacco use, the random-effects estimate was 1.87 (95% confidence interval 1.40-2.48). The increase was mainly evident in studies conducted before 1980. No increase was seen in studies in Scandinavia. Restricting attention to the seven estimates adjusted for smoking and alcohol eliminated both heterogeneity and excess risk (1.02; 0.82-1.28). Estimates also varied by sex (higher in females) and by study design (higher in case-control studies with hospital controls) but more clearly in studies where estimates were unadjusted, even for age. The pattern of estimates suggests some publication bias. Based on limited data specific to never smokers, the random-effects estimate was 1.94 (0.88-4.28), the eight individual estimates being heterogeneous and based on few exposed cases.
Conclusion: Smokeless tobacco, as used in America or Europe, carries at most a minor increased risk of oral cancer. However, elevated risks in specific populations or from specific products cannot definitely be excluded.
Figures
Comment in
-
Oral cancer risk and smokeless tobacco products--clouded by smoke?Evid Based Dent. 2008;9(4):114-5. doi: 10.1038/sj.ebd.6400615. Evid Based Dent. 2008. PMID: 19151684
References
-
- World Health Organization . International statistical classification of diseases and related health problems Tenth revision. Vol. 1. Geneva: WHO; 1992. - PubMed
-
- International Agency for Research on Cancer Globocan 2002 database project. 2002. http://www-dep.iarc.fr/
-
- American Cancer Society All about oral cavity and oropharyngeal cancer. 2005. http://www.cancer.org/docroot/CRI/CRI_2x.asp?sitearea=&dt=60
-
- World Health Organization WHO statistical information system (WHOSIS) 2005. http://www.who.int/whosis
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
