

Insights into normal and disordered bowel habits from bowel diaries
- PMID: 18021288
- PMCID: PMC2557101
- DOI: 10.1111/j.1572-0241.2007.01631.x
Insights into normal and disordered bowel habits from bowel diaries
Abstract
Background: While symptom questionnaires provide a snapshot of bowel habits, they may not reflect day-to-day variations or the relationship between bowel symptoms and stool form.
Aim: To assess bowel habits by daily diaries in women with and without functional bowel disorders.
Method: From a community-based survey among Olmsted County, MN, women, 278 randomly selected subjects were interviewed by a gastroenterologist, who completed a bowel symptom questionnaire. Subjects also maintained bowel diaries for 2 wk.
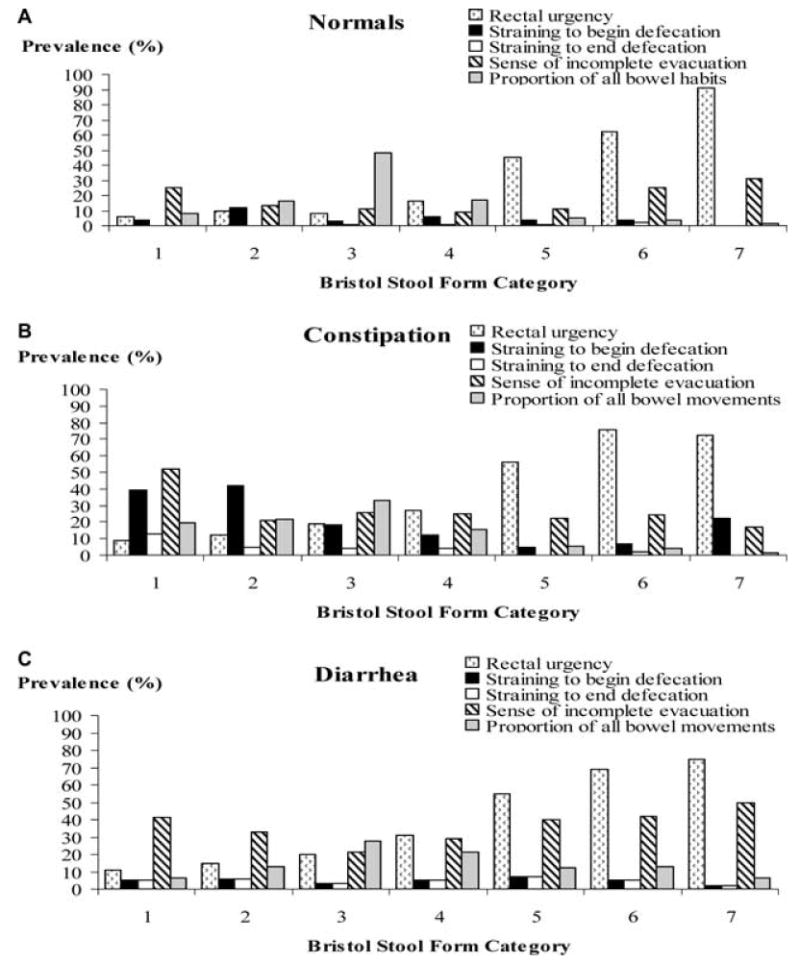
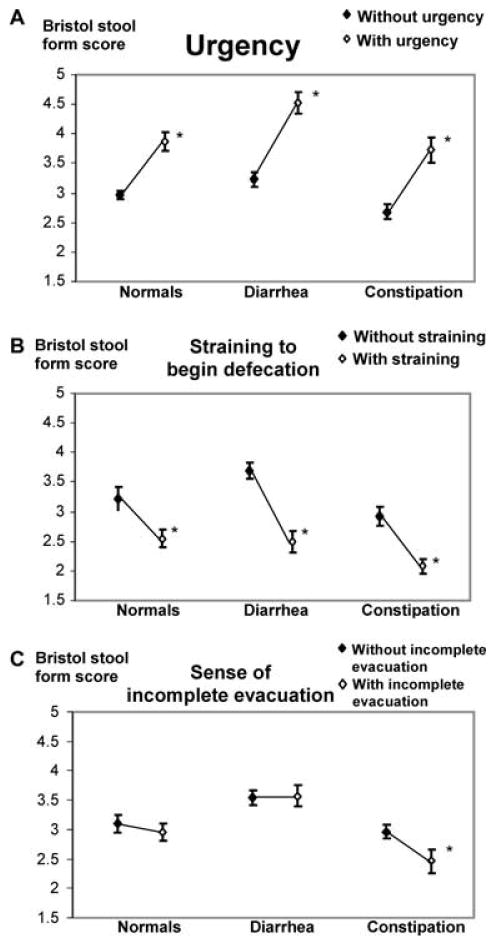
Results: Among 278 subjects, questionnaires revealed diarrhea (26%), constipation (21%), or neither (53%). Asymptomatic subjects reported bowel symptoms (e.g., urgency) infrequently (i.e., <25% of the time) and generally for hard or loose stools. Urgency for soft, formed stools (i.e., Bristol form = 4) was more prevalent in subjects with diarrhea (31%) and constipation (27%) than in normals (16%). Stool form, straining to begin (odds ratio [OR] 4.1, 95% confidence interval [CI] 1.7-10.2) and end (OR 4.7, 95% CI 1.6-15.2) defecation increased the odds for constipation. Straining to end defecation (OR 3.7, 95% CI 1.2-12.0), increased stool frequency (OR 1.9, 95% CI 1.02-3.7), incomplete evacuation (OR 2.2, 95% CI 1.04-4.6), and rectal urgency (OR 3.1, 95% CI 1.4-6.6) increased the odds for diarrhea. In contrast, variations in stool frequency and form were not useful for discriminating between health and disease.
Conclusions: Bowel symptoms occur in association with, but are only partly explained by, stool form disturbances. These observations support a role for other pathophysiological mechanisms in functional bowel disorders.
Conflict of interest statement
Figures
References
-
- Cremonini F, Talley NJ. Irritable bowel syndrome: Epidemiology, natural history, health care seeking and emerging risk factors. Gastroenterology Clinics of North America. 2005;34:189–204. - PubMed
-
- Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480–91. erratum appears in Gastroenterology. 2006;131(2):688. - PubMed
-
- Chaussade S, Khyari A, Roche H, et al. Determination of total and segmental colonic transit time in constipated patients. Results in 91 patients with a new simplified method. Dig Dis Sci. 1989;34:1168–72. - PubMed
-
- Ashraf W, Park F, Lof J, et al. An examination of the reliability of reported stool frequency in the diagnosis of idiopathic constipation. Am J Gastroenterol. 1996;91:26–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
