

Evaluation of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery in a series of pediatric patients
- PMID: 18021877
- PMCID: PMC2140045
- DOI: 10.1016/j.jacc.2007.06.055
Evaluation of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery in a series of pediatric patients
Abstract
Objectives: We sought to prospectively evaluate evidence of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery with an interarterial course (AAOCA).
Background: An AAOCA is a rare anomaly associated with increased myocardial ischemia and sudden death risk in children. Data evaluating ischemia after AAOCA repair are limited.
Methods: We included children who underwent AAOCA surgery between October 2001 and December 2006. They were prospectively assessed with exercise stress test (EST), stress echocardiogram (SE), and stress myocardial perfusion scan (MPS).
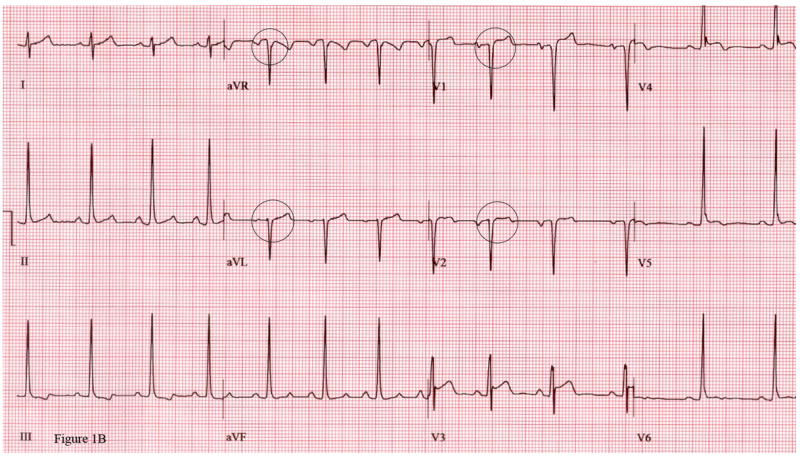
Results: Of 24 participating children, 15 (63%) were male, 16 (67%) had anomalous right coronary (ARCA), and 7 (29%) were asymptomatic. Median age was 12 (5 to 18) years; follow-up was 15 (2 to 48) months. All had unobstructed neo-coronary ostia by echocardiogram and were asymptomatic. One anomalous origin of left main coronary artery (ALCA) patient and 8 ARCA patients had post-operative evaluations suggestive of ischemia. The ALCA patient had reversible apical septal and mid-anteroseptal hypokinesis on SE. Of the ARCA patients, 2 had inferior ST-segment depression on EST; subsequently, 1 had normal tests, but the other developed anterolateral Q waves. Two patients had blunted blood pressure response with EST, 1 had fixed apical inferior hypokinesis on SE, 2 had reversible perfusion defects on MPS, and 1 had a fixed perfusion defect on MPS.
Conclusions: Subclinical changes suggestive of ischemia might occur despite patent neo-coronary ostia, notably after ARCA repair. The implication of these results on indication for surgery and subsequent sudden death risk is unknown. Serial EST, SE, and MPS are essential in evaluating ongoing ischemia risk after AAOCA repair.
Conflict of interest statement
There are no Conflicts of Interest
Figures

Comment in
-
Management of anomalous coronary artery from the contralateral coronary sinus.J Am Coll Cardiol. 2007 Nov 20;50(21):2083-4. doi: 10.1016/j.jacc.2007.08.023. Epub 2007 Nov 5. J Am Coll Cardiol. 2007. PMID: 18021878 No abstract available.
References
-
- Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol. 1992;20:640–7. - PubMed
-
- Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000;35:1493–501. - PubMed
-
- Frescura C, Basso C, Thiene G, et al. Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Hum Pathol. 1998;29:689–95. - PubMed
-
- Kragel AH, Roberts WC. Anomalous origin of either the right or left main coronary artery from the aorta with subsequent coursing between aorta and pulmonary trunk: analysis of 32 necropsy cases. Am J Cardiol. 1988;62:771–7. - PubMed
-
- Corrado D, Thiene G, Nava A, Rossi L, Pennelli N. Sudden death in young competitive athletes: clinicopathologic correlations in 22 cases. Am J Med. 1990;89:588–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
