

Prognostic value of lateral lymph node metastasis for advanced low rectal cancer
- PMID: 18023098
- PMCID: PMC4250889
- DOI: 10.3748/wjg.v13.45.6048
Prognostic value of lateral lymph node metastasis for advanced low rectal cancer
Abstract
Aim: To evaluate the risk factors for lateral lymph node metastasis in patients with advanced low rectal cancer, in order to make the effective selection of patients who could benefit from lateral lymph node dissection, as well as the relationship of lateral lymph node metastasis with local recurrence and survival of patients with advanced low rectal cancer.
Methods: A total of 96 consecutive patients who underwent curative surgery with lateral pelvic lymphadenectomy for advanced lower rectal cancer were retrospectively analyzed. The relation of lateral lymph node metastasis with clinicopathologic characteristics, local recurrence and survival of patients was identified.
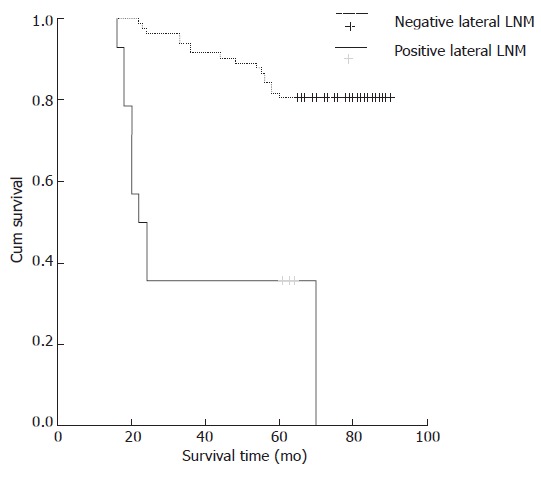
Results: Lateral lymph node metastasis was observed in 14.6% (14/96) of patients with advanced low rectal cancer. Lateral lymph node metastasis was detected in 10 (25.0%) of 40 patients with tumor diameter >or= 5 cm and in 4 (7.1%) of 56 patients with tumor diameter < 5 cm. The difference between the two groups was statistically significant (c2 = 5.973, P = 0.015). Lateral lymph node metastasis was more frequent in patients with 4/4 diameter of tumor infiltration (7 of 10 cases, 70.0%), compared with patients with 3/4, 2/4 and 1/4 diameter of tumor infiltration (3 of 25 cases, 12.0%; 3 of 45 cases, 6.7%; 1 of 16 cases, 6.3%) (c2 = 27.944, P = 0.0001). The lateral lymph node metastasis rate was 30.0% (9 of 30 cases), 9.1% (4 of 44 cases) and 4.5% (1 of 22 cases) for poorly, moderately and well-differentiated carcinoma, respectively. The difference between the three groups was statistically significant (c2 = 8.569, P = 0.014). Local recurrence was 18.8% (18 of 96 cases), 64.3% (9 of 14 cases), and 11.0% (9 of 82 cases) in patients with advanced low rectal cancer, in those with and without lateral lymph node metastasis, respectively. The difference between the two groups was statistically significant (c2 = 22.308, P = 0.0001). Kaplan-Meier survival analysis showed significant improvements in median survival (80.9 +/- 2.1 m, 95% CI: 76.7-85.1 m vs 38 +/- 6.7 m, 95% CI: 24.8-51.2 m) of patients without lateral lymph node metastasis compared with those with lateral lymph node metastasis (log-rank, P = 0.0001).
Conclusion: Tumor diameter, infiltration and differentiation are significant risk factors for lateral lymph node metastasis. Lateral pelvic lymphadenectomy should be performed following surgery for patients with tumor diameter >or= 5 cm. Lateral lymph node metastasis is an important predictor for local recurrence and survival in patients with advanced low rectal cancer.
Figures
References
-
- Laurent C, Nobili S, Rullier A, Vendrely V, Saric J, Rullier E. Efforts to improve local control in rectal cancer compromise survival by the potential morbidity of optimal mesorectal excision. J Am Coll Surg. 2006;203:684–691. - PubMed
-
- Bernardshaw SV, Øvrebø K, Eide GE, Skarstein A, Røkke O. Treatment of rectal cancer: reduction of local recurrence after the introduction of TME - experience from one University Hospital. Dig Surg. 2006;23:51–59. - PubMed
-
- Liang YC, Qing SH, Ding WX, Chen PY, Huang YB, Yu HT. Total mesorectal excision versus conventional radical surgery for rectal cancer: a meta analysis. Zhonghua Weichangwaike Zazhi. 2007;10:43–48. - PubMed
-
- Tzardi M. Role of total mesorectal excision and of circumferential resection margin in local recurrence and survival of patients with rectal carcinoma. Dig Dis. 2007;25:51–55. - PubMed
-
- Wibe A, Eriksen MT, Syse A, Myrvold HE, Søreide O. Total mesorectal excision for rectal cancer--what can be achieved by a national audit? Colorectal Dis. 2003;5:471–477. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
