Investigation of biofilm formation in clinical isolates of Staphylococcus aureus
- PMID: 18025674
- PMCID: PMC4098860
- DOI: 10.1007/978-1-59745-468-1_10
Investigation of biofilm formation in clinical isolates of Staphylococcus aureus
Abstract
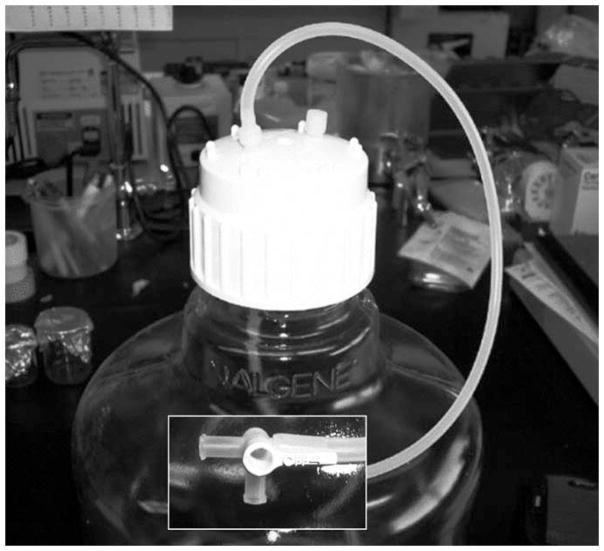
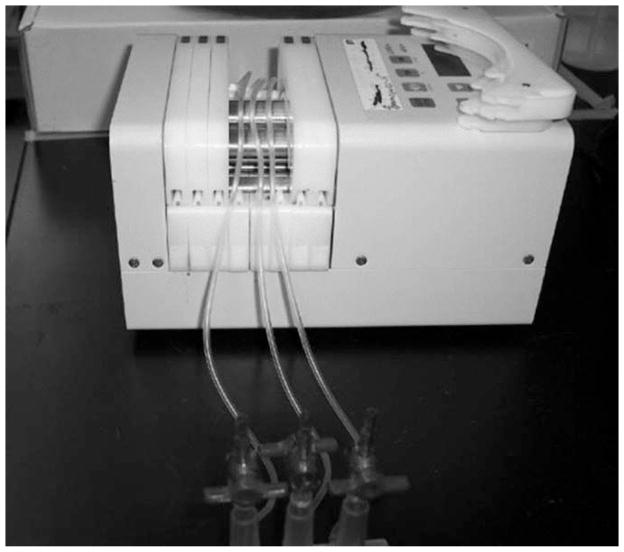
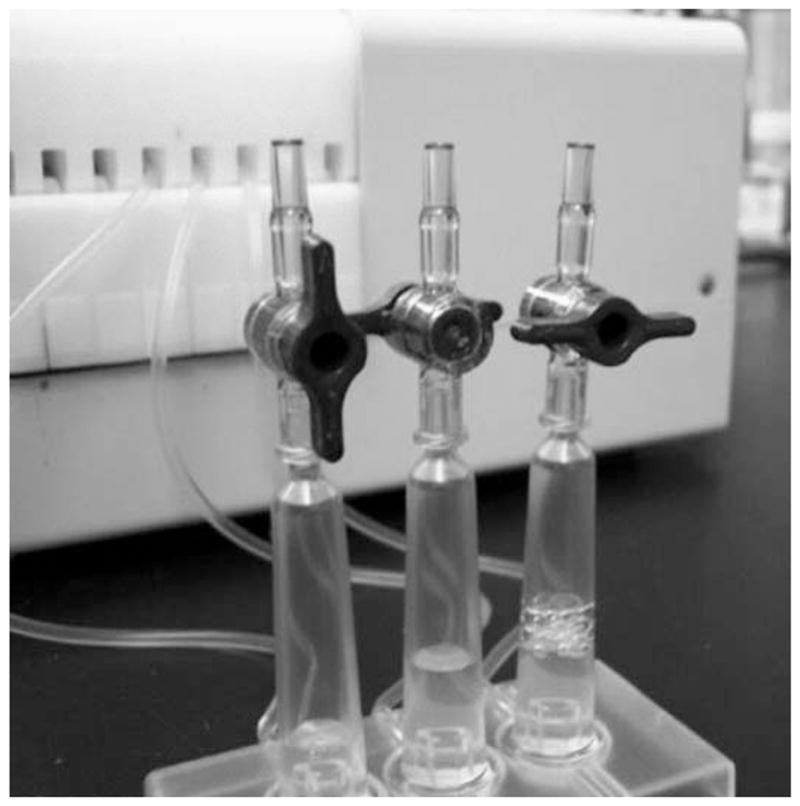
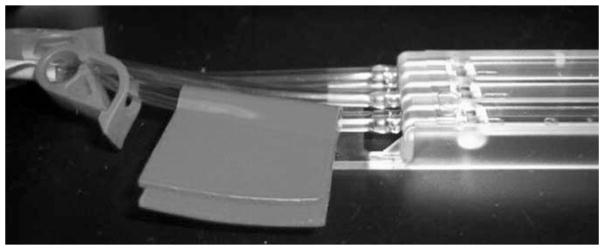
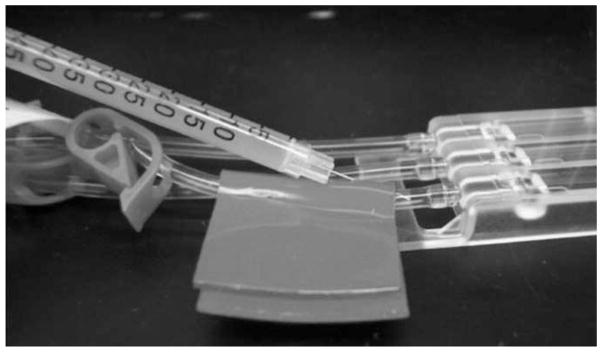
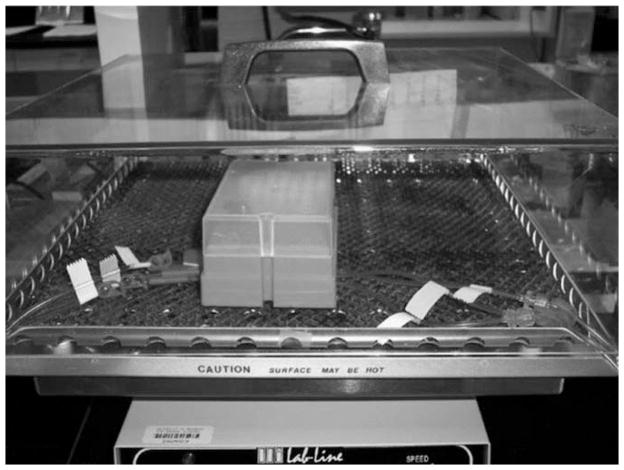
As with many other bacterial species, the most commonly used method to assess staphylococcal biofilm formation in vitro is the microtiter plate assay. This assay is particularly useful for comparison of multiple strains including large-scale screens of mutant libraries. When such screens are applied to the coagulase-negative staphylococci in general, and Staphylococcus epidermidis in particular, they are relatively straightforward by comparison with microtiter plate assays used to assess biofilm formation in other bacterial species. However, in the case of clinical isolates of Staphylococcus aureus, including methicillin-resistant S. aureus, we have found it necessary to employ specific modifications including precoating of the wells of the microtiter plate with plasma proteins and supplementation of the medium with both salt and glucose. In this chapter, we describe the microtiter plate assay in the specific context of clinical isolates of S. aureus and the use of these modifications. A second in vitro method, which also is generally dependent on coating with plasma proteins and supplementation of the growth medium, is the use of flow cells. In this method, bacteria are allowed to attach to a surface and then monitored with respect to their ability to remain attached to the substrate and differentiate into mature biofilms under the constant pressure of fluid shear force. Although flow cells are not applicable to large-scale screens, we have found that they provide a more reproducible and accurate assessment of the capacity of S. aureus clinical isolates to form a biofilm. They also provide a means of analyzing structural differences in biofilm architecture and isolating bacteria and/or spent media for analysis of physiological and metabolic changes associated with the adaptive response to growth in a biofilm. While a primary focus of this chapter is on the use of in vitro assays to assess biofilm formation in clinical isolates of S. aureus, it is important to emphasize two additional considerations. First, it has become increasingly evident that biofilm formation in S. epiderimidis and S. aureus is not equivalent. Additionally, to date, most studies with S. aureus have been done with a very limited number of strains, almost all of which are derived from the NCTC strain designated 8325, and we have found that these strains are not representative of the most relevant clinical isolates. As with the specific elements of our flow cell system, we have written this chapter to reflect our focus on clinical isolates of S. aureus and the specific methods that we have found most reliable in that context. Second, as is often the case, in vitro methods do not necessarily reflect events that occur in vivo. Several in vivo methods to assess biofilm formation have been described, and these generally fall into one of two categories. The first focuses directly on staphylococcal diseases that are generally thought to include a biofilm component (e.g., endocarditis, osteomyelitis, septic arthritis). A discussion of these models is also beyond the scope of this chapter, but examples are easily found in the staphylococcal literature. The second approach uses some form of implanted device in an attempt to focus more directly on implant-associated biofilms. We use a model in which a small piece of Teflon catheter is implanted subcutaneously in mice and used as a substrate for colonization. We have the advantage of using bioluminescent derivatives of S. aureus clinical isolates and the IVIS(R) imaging system. However, because this system is not generally available, we restrict technical comments in this chapter to our use of an implanted catheter model evaluated by direct microbio-logical analysis of explanted catheters (2).
Figures


References
-
- Keren I, Kaldalu N, Spoering A, Wang Y, Lewis K. Persister cells and tolerance to antimicrobials. FEMS Microbiol Lett. 2004;230:13–18. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials