

A randomized pilot validation of educational measures in teaching shoulder arthroscopy to surgical residents
- PMID: 18031640
- PMCID: PMC2386192
A randomized pilot validation of educational measures in teaching shoulder arthroscopy to surgical residents
Abstract
Background: Injuries to the shoulder joint commonly require the attention of an orthopedic surgeon. Shoulder arthroscopy plays an increasingly important role in the diagnosis and repair of shoulder pathology; however, the most effective manner in which to teach orthopedic residents fundamental knowledge of diagnostic shoulder arthroscopy before entering the operating room is unclear. We aimed to compare the existing cadaver-based teaching of diagnostic shoulder arthroscopy knowledge with a method that combines model- and video-based teaching to orthopedic surgery residents in a randomized pilot trial.
Methods: A composite (model/video teaching) method was designed, using prepared teaching videos and the commercially available ALEX shoulder arthroscopy model. First- and second-year orthopedic surgery residents from the University of Calgary were consented, surveyed for their arthroscopy experience and randomized to either cadaver or composite teaching. Subjects wrote a pretest before their teaching session and a posttest afterwards to assess their knowledge of diagnostic arthroscopy. The tests were multiple choice, containing text and pictorial-based questions. The posttest was modified to minimize recall bias. Subjects were also surveyed for their comments regarding the teaching sessions.
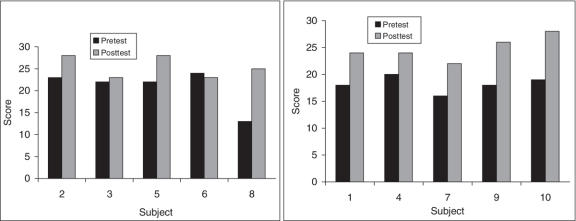
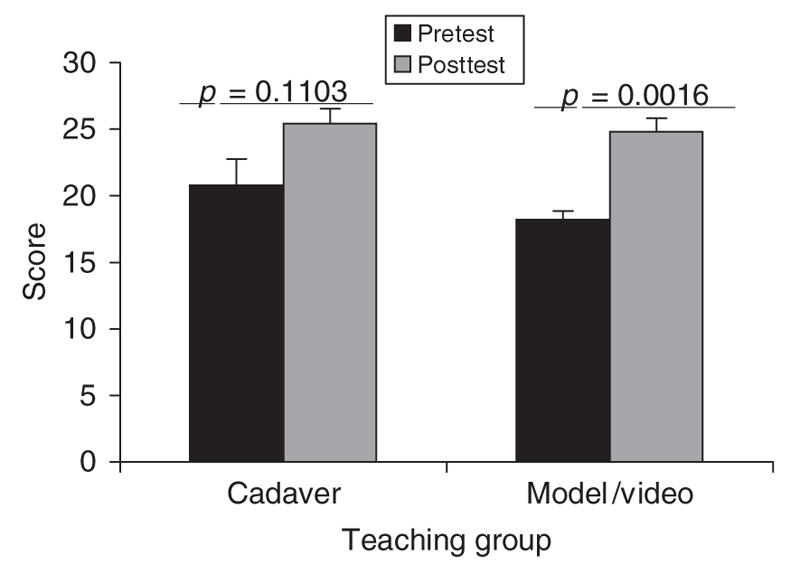
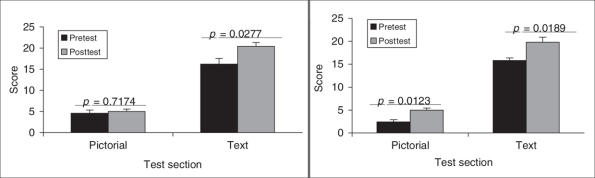
Results: Nine of 10 subjects increased their test scores after the teaching sessions, with 4 of 5 in the cadaver-based and 5 of 5 in the composite groups. There were no differences between the teaching groups on their mean pre- or posttest scores. The composite group, but not the cadaver-based group, had a statistically significant increase in posttest scores. When the text- and pictorial-based question sections were analyzed separately, both groups significantly improved their mean text-based score, whereas only the composite group increased their mean pictorial-based questions score. Surveying the residents elicited positive comments regarding both manners of teaching.
Conclusion: This pilot trial suggests that a composite teaching curriculum is at least as effective as a cadaver-based environment for teaching orthopedic surgery residents fundamental knowledge of diagnostic shoulder arthroscopy.
Contexte: Les blessures à l'articulation de l'épaule exigent souvent l'intervention d'un chirurgien orthopédiste. L'arthroscopie de l'épaule joue un rôle de plus en plus important dans le diagnostic et la correction des pathologies de l'épaule, mais ne sait pas clairement quelle est la façon la plus efficace d'enseigner aux résidents en orthopédie les bases de l'arthroscopie diagnostique de l'épaule avant d'entrer en salle d'opération. Nous voulions comparer au moyen d'une étude pilote randomisée la façon actuelle d'enseigner à des résidents en chirurgie orthopédique l'arthroscopie diagnostique de l'épaule sur cadavres à une méthode qui combine un enseignement sur modèle et une formation vidéo.
Méthodes: On a conçu une méthode composée (enseignement sur modèle et formation vidéo) fondée sur des vidéos didactiques préparées et sur le modèle commercial d'arthroscopie de l'épaule ALEX. On a obtenu le consentement de résidents de première et de deuxième année en chirurgie orthopédique de l'Université de Calgary, on les a interrogés pour déterminer leur expérience de l'arthroscopie et on les a affectés par randomisation à la méthode de formation sur cadavre ou à la méthode composée. Les sujets se sont soumis à un pré-test avant leur séance de formation et à un post-test par la suite pour évaluer leur connaissance de l'arthroscopie diagnostique. Les tests à choix multiples contenaient des questions à base de texte et d'éléments graphiques. On a modifié le post-test pour réduire le plus possible le biais attribuable à la mémoire. On a aussi demandé aux sujets de commenter les séances de formation.
Résultats: Neuf des 10 sujets ont amélioré leurs résultats de tests après les séances de formation, soit 4 des 5 qui ont reçu une formation sur cadavre et 5 des 5 qui ont reçu la formation composée. Les résultats moyens au pré-test ou au post-test ne différaient pas entre les groupes. Chez les sujets qui ont reçu la formation composée, mais non chez ceux qui ont reçu la formation sur cadavres, les résultats au post-test ont augmenté de façon statistiquement significative. Lorsqu'on a analysé séparément les questions à base de texte et d'éléments graphiques, on a constaté que les deux groupes ont amélioré de façon significative leurs résultats moyens aux questionnaires à base de texte, tandis que seuls les sujets qui ont reçu la formation composée ont amélioré leurs résultats moyens aux questions à base d'éléments graphiques. Le sondage auprès des résidents a suscité des commentaires positifs au sujet des deux méthodes de formation.
Conclusion: Cette étude pilote indique qu'un programme de formation composée est au moins aussi efficace qu'une formation sur cadavres pour inculquer aux résidents en chirurgie orthopédique les bases de l'arthroscopie diagnostique de l'épaule.
Figures

Similar articles
-
Arthroscopy skills development with a surgical simulator: a comparative study in orthopaedic surgery residents.Am J Sports Med. 2015 Jun;43(6):1526-9. doi: 10.1177/0363546515574064. Epub 2015 Mar 13. Am J Sports Med. 2015. PMID: 25769535 Clinical Trial.
-
A Checklist Intervention to Assess Resident Diagnostic Knee and Shoulder Arthroscopic Efficiency.J Surg Educ. 2017 Jan-Feb;74(1):9-15. doi: 10.1016/j.jsurg.2016.07.007. Epub 2016 Aug 23. J Surg Educ. 2017. PMID: 27561628
-
Improving Resident Performance in Knee Arthroscopy: A Prospective Value Assessment of Simulators and Cadaveric Skills Laboratories.J Bone Joint Surg Am. 2016 Feb 3;98(3):220-5. doi: 10.2106/JBJS.O.00440. J Bone Joint Surg Am. 2016. PMID: 26842412
-
Teaching hip surgery to orthopaedic residents: what's new?Hip Int. 2020 Sep;30(1_suppl):42-47. doi: 10.1177/1120700020916451. Hip Int. 2020. PMID: 32907428 Review.
-
Shoulder arthroscopy in children and adolescents.J Am Acad Orthop Surg. 2013 Jul;21(7):389-97. doi: 10.5435/JAAOS-21-07-389. J Am Acad Orthop Surg. 2013. PMID: 23818026 Review.
Cited by
-
Shoulder Arthroscopy Simulator Training Improves Surgical Procedure Performance: A Controlled Laboratory Study.Orthop J Sports Med. 2021 May 10;9(5):23259671211003873. doi: 10.1177/23259671211003873. eCollection 2021 May. Orthop J Sports Med. 2021. PMID: 33997080 Free PMC article.
-
Orthopedic surgery residents' perception of online education in their programs during the COVID-19 pandemic: should it be maintained after the crisis?Acta Orthop. 2020 Oct;91(5):543-546. doi: 10.1080/17453674.2020.1776461. Epub 2020 Jun 15. Acta Orthop. 2020. PMID: 32539473 Free PMC article.
-
Impact of urology simulation boot camp in improving endoscopic instrument knowledge.BMJ Simul Technol Enhanc Learn. 2018 Jul 11;5(3):151-154. doi: 10.1136/bmjstel-2018-000313. eCollection 2019. BMJ Simul Technol Enhanc Learn. 2018. PMID: 35514940 Free PMC article.
-
Development of simulated arthroscopic skills.Acta Orthop. 2011 Feb;82(1):90-5. doi: 10.3109/17453674.2011.552776. Epub 2011 Feb 1. Acta Orthop. 2011. PMID: 21281257 Free PMC article. Clinical Trial.
-
E-learning in orthopedic surgery training: A systematic review.J Orthop. 2016 Sep 21;13(4):425-30. doi: 10.1016/j.jor.2016.09.004. eCollection 2016 Dec. J Orthop. 2016. PMID: 27688638 Free PMC article. Review.
References
-
- Schappert SM. Office visits to orthopedic surgeons: United States, 1995-1996. Adv Data 1998;302:1-32. - PubMed
-
- Mohtadi NG, Vellet AD, Clark ML, et al. A prospective, double-blind comparison of magnetic resonance imaging and arthro-scopy in the evaluation of patients presenting with shoulder pain. J Shoulder Elbow Surg 2004;13:258-65. - PubMed
-
- Angelo RL. Controversies in arthroscopic shoulder surgery: arthroscopic repair versus open Bankart repair, thermal treatment of capsular tissue, acromioplasties —are they necessary? Arthroscopy 2003;19(Suppl 2):224-32. - PubMed
-
- Millstein ES, Snyder SJ. Arthroscopic management of partial, full-thickness, and complex rotator cuff tears: indication, techniques and complications. Arthroscopy 2003;19(Suppl 1):189-99. - PubMed
-
- Fabbriciani C, Milano G, Demontis A, et al. Arthroscopic versus open treatment of Bankart lesion of the shoulder: a prospective randomized study. Arthroscopy 2004;20:456-62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources