

Phase I trial of a CD8+ T-cell peptide epitope-based vaccine for infectious mononucleosis
- PMID: 18032491
- PMCID: PMC2224445
- DOI: 10.1128/JVI.01409-07
Phase I trial of a CD8+ T-cell peptide epitope-based vaccine for infectious mononucleosis
Abstract
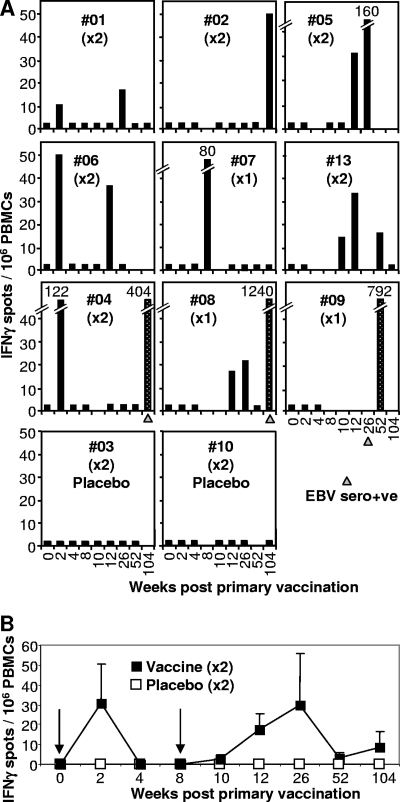
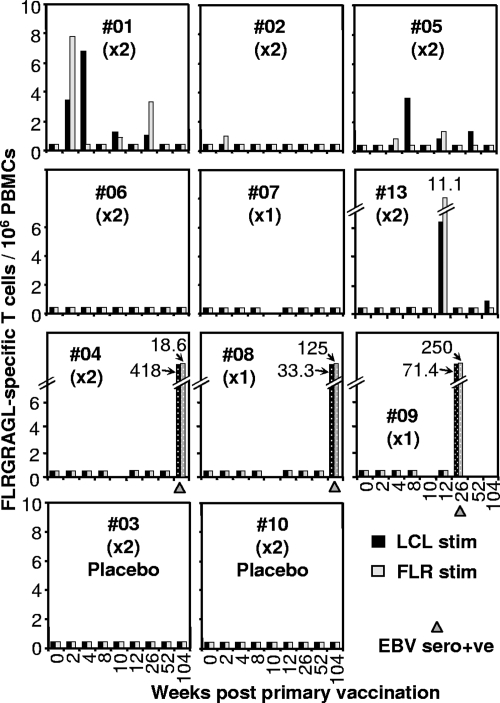
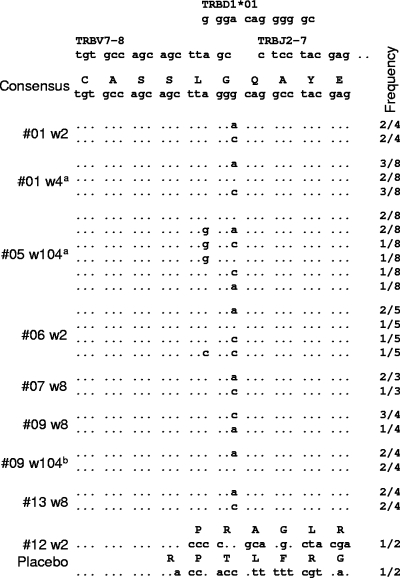
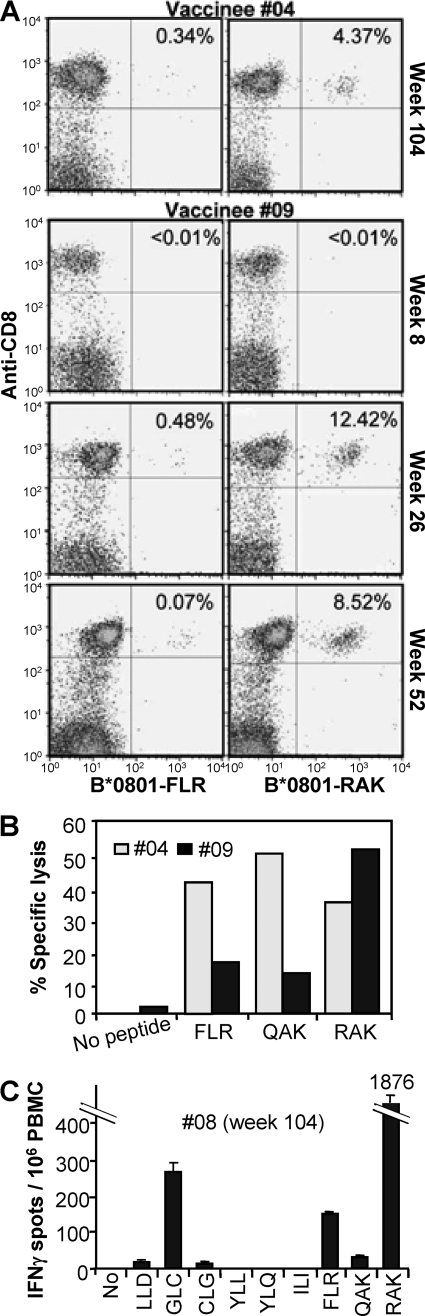
A single blind, randomized, placebo-controlled, single-center phase I clinical trial of a CD8(+) T-cell peptide epitope vaccine against infectious mononucleosis was conducted with 14 HLA B*0801-positive, Epstein-Barr virus (EBV)-seronegative adults. The vaccine comprised the HLA B*0801-restricted peptide epitope FLRGRAYGL and tetanus toxoid formulated in a water-in-oil adjuvant, Montanide ISA 720. FLRGRAYGL-specific responses were detected in 8/9 peptide-vaccine recipients and 0/4 placebo vaccine recipients by gamma interferon enzyme-linked immunospot assay and/or limiting-dilution analysis. The same T-cell receptor Vbeta CDR3 sequence that is found in FLRGRAYGL-specific T cells from most EBV-seropositive individuals could also be detected in the peripheral blood of vaccine recipients. The vaccine was well tolerated, with the main side effect being mild to moderate injection site reactions. After a 2- to 12-year follow-up, 1/2 placebo vaccinees who acquired EBV developed infectious mononucleosis, whereas 4/4 vaccinees who acquired EBV after completing peptide vaccination seroconverted asymptomatically. Single-epitope vaccination did not predispose individuals to disease, nor did it significantly influence development of a normal repertoire of EBV-specific CD8(+) T-cell responses following seroconversion.
Figures
References
-
- Adams, L. A., B. Deboer, G. Jeffrey, R. Marley, and G. Garas. 2006. Ganciclovir and the treatment of Epstein-Barr virus hepatitis. J. Gastroenterol. Hepatol. 211758-1760. - PubMed
-
- Aichele, P., K. Brduscha-Riem, S. Oehen, B. Odermatt, R. M. Zinkernagel, H. Hengartner, and H. Pircher. 1997. Peptide antigen treatment of naive and virus-immune mice: antigen-specific tolerance versus immunopathology. Immunity 6519-529. - PubMed
-
- Argaet, V. P., C. W. Schmidt, S. R. Burrows, S. L. Silins, M. G. Kurilla, D. L. Doolan, A. Suhrbier, D. J. Moss, E. Kieff, T. B. Sculley, and I. S. Misko. 1994. Dominant selection of an invariant T cell antigen receptor in response to persistent infection by Epstein-Barr virus. J. Exp. Med. 1802335-2340. - PMC - PubMed
-
- Bharadwaj, M., S. R. Burrows, J. M. Burrows, D. J. Moss, M. Catalina, and R. Khanna. 2001. Longitudinal dynamics of antigen-specific CD8+ cytotoxic T lymphocytes following primary Epstein-Barr virus infection. Blood 982588-2589. - PubMed
-
- Bharadwaj, M., M. Sherritt, R. Khanna, and D. J. Moss. 2001. Contrasting Epstein-Barr virus-specific cytotoxic T cell responses to HLA A2-restricted epitopes in humans and HLA transgenic mice: implications for vaccine design. Vaccine 193769-3777. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
