

Atrophy rates accelerate in amnestic mild cognitive impairment
- PMID: 18032747
- PMCID: PMC2734477
- DOI: 10.1212/01.wnl.0000281688.77598.35
Atrophy rates accelerate in amnestic mild cognitive impairment
Abstract
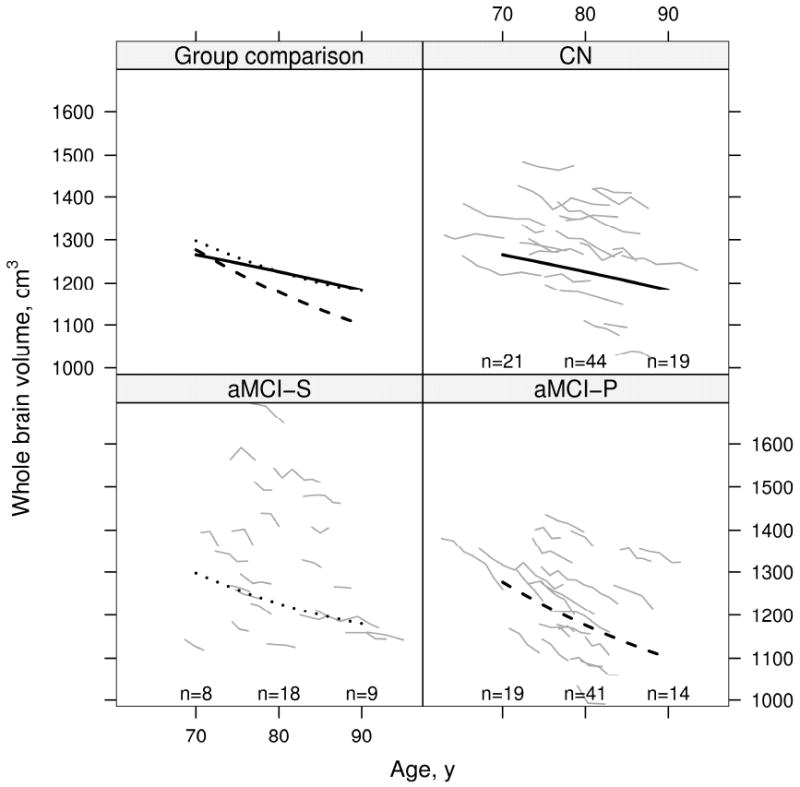
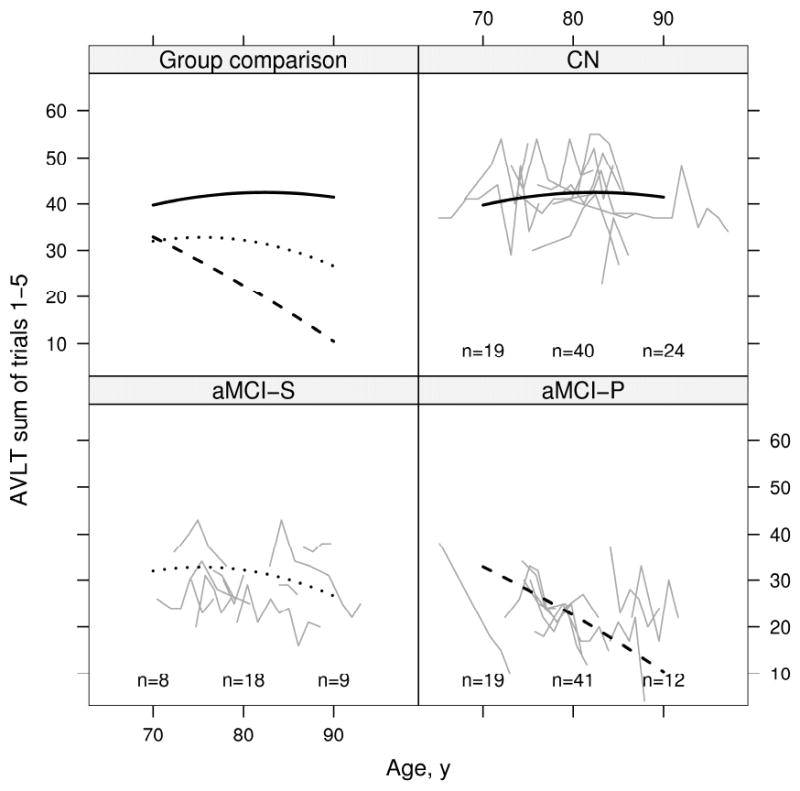
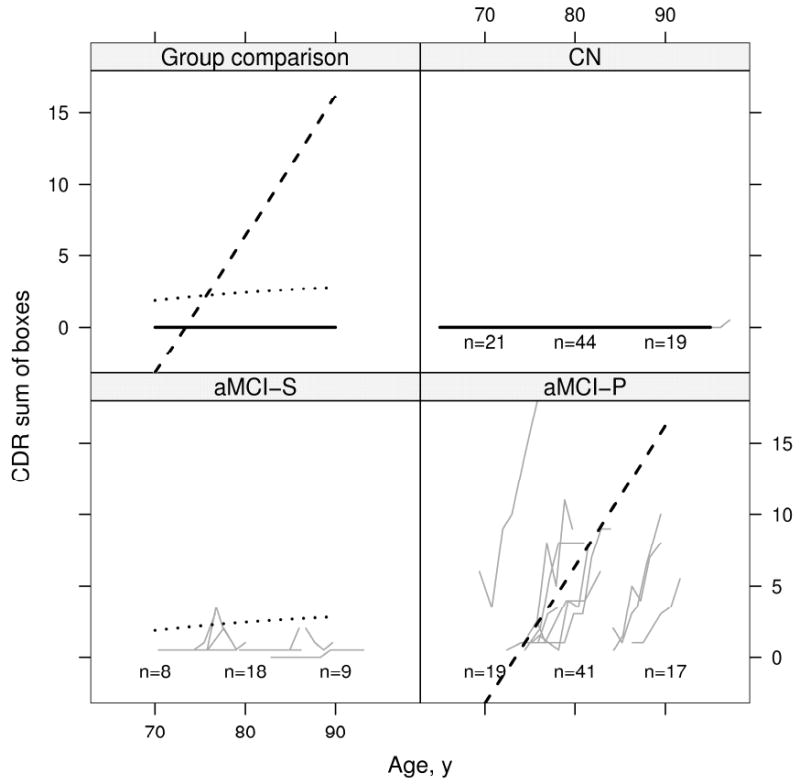
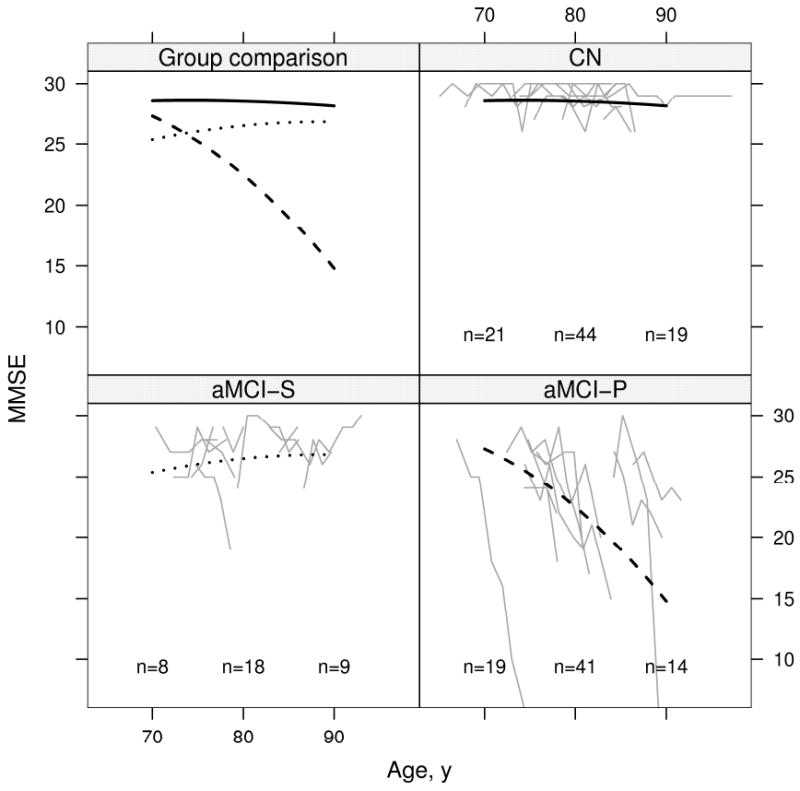
Background: We tested if rates of brain atrophy accelerate in individuals with amnestic mild cognitive impairment (aMCI) as they progress to typical late onset Alzheimer disease (AD). We included comparisons to subjects with aMCI who did not progress (labeled aMCI-S) and also to cognitively normal elderly subjects (CN).
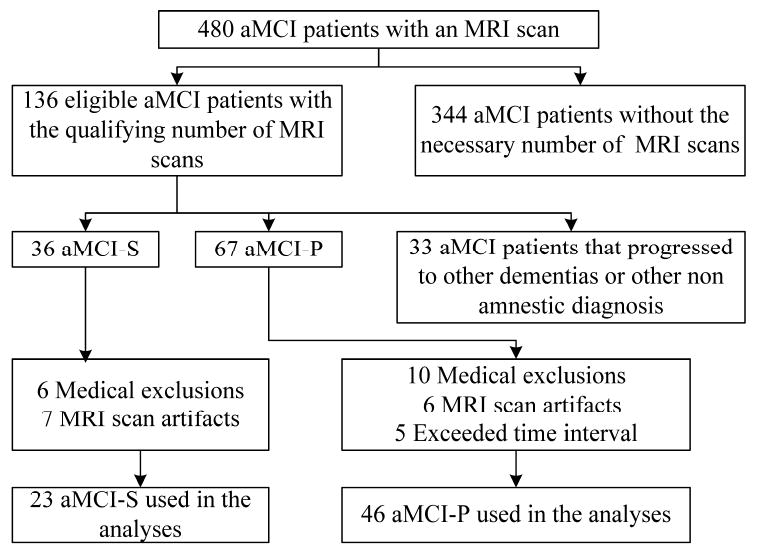
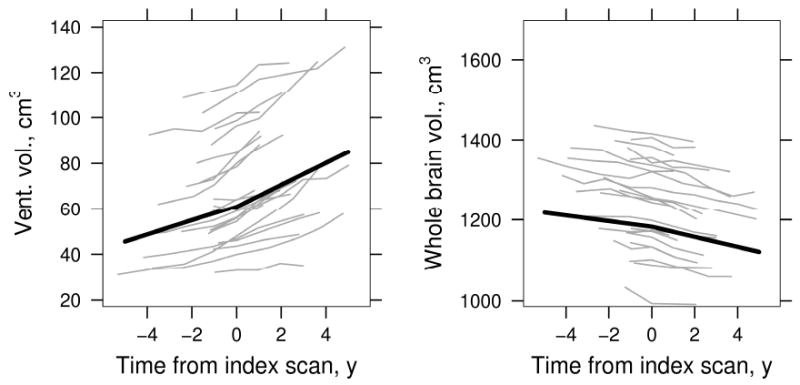
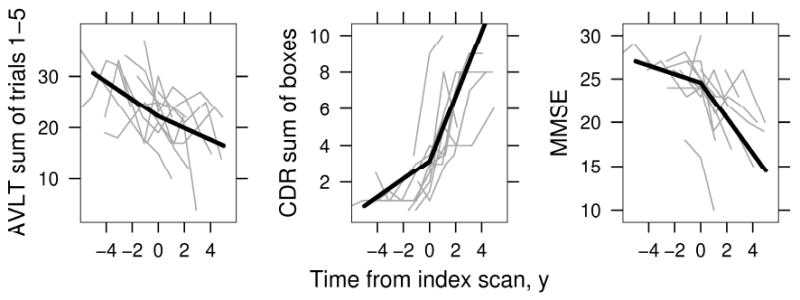
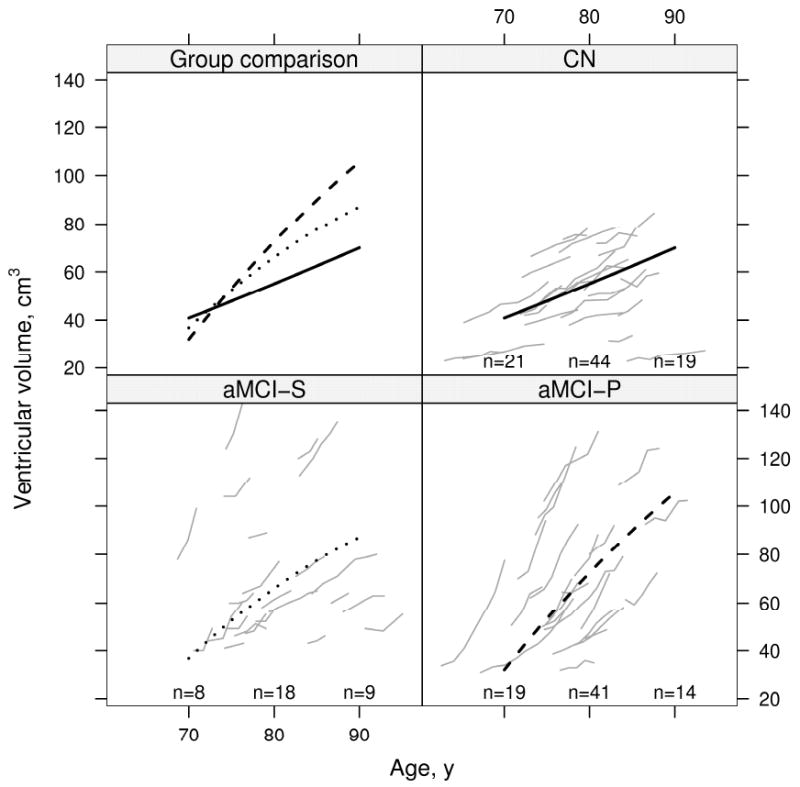
Methods: We studied 46 subjects with aMCI who progressed to AD (labeled aMCI-P), 46 CN, and 23 aMCI-S. All subjects must have had three or more serial MRI scans. Rates of brain shrinkage and ventricular expansion were measured across all available serial MRI scans in each subject. Change in volumes relative to the point at which subjects progressed to a clinical diagnosis of AD (the index date) was modeled in aMCI-P. Change in volumes relative to age was modeled in all three clinical groups.
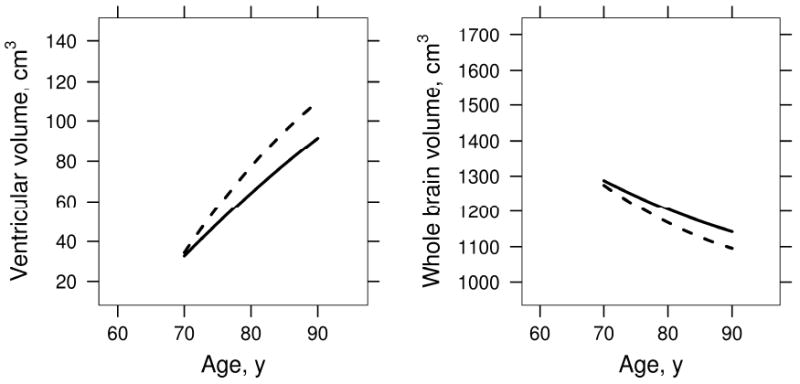
Results: In aMCI-P the change in pre to post index rate (i.e., acceleration) of ventricular expansion was 1.7 cm(3)/year, and acceleration in brain shrinkage was 5.3 cm(3)/year. Brain volume declined and ventricular volume increased in all three groups with age. Volume changes decelerated with increasing age in aMCI-P, and to a lesser extent in aMCI-S, but were linear in the matched CN. Among all subjects with aMCI, rates of atrophy were greater in apolipoprotein E epsilon 4 carriers than noncarriers.
Conclusions: Rates of atrophy accelerate as individuals progress from amnestic mild cognitive impairment (aMCI) to typical late onset Alzheimer disease (AD). Rates of atrophy are greater in younger than older subjects with aMCI who progressed to AD and subjects with aMCI who did not progress. We did not find that atrophy rates varied with age in 70- to 90-year-old cognitively normal subjects.
Figures
Comment in
-
Atrophy accelerates with conversion from mild cognitive impairment to Alzheimer disease.Neurology. 2008 May 6;70(19 Pt 2):1728-9. doi: 10.1212/01.wnl.0000311448.61194.0f. Neurology. 2008. PMID: 18458214 No abstract available.
References
-
- Braak H, Braak E, Bohl J. Staging of Alzheimer-related cortical destruction. Eur Neurol. 1993;33:403–408. - PubMed
-
- Hyman B. The neuropathological diagnosis of Alzheimer's disease: clinical-pathological studies. Neurobiology of Aging. 1997;18(4 Suppl):S27–32. - PubMed
-
- Terry RD, Masliah E, Salmon DP, et al. Physical basis of cognitive alterations in Alzheimer's disease: synapse loss is the major correlate of cognitive impairment. Ann Neurol. 1991;30:572–580. - PubMed
-
- Fox NC, Warrington EK, Freeborough PA, et al. Presymptomatic hippocampal atrophy in Alzheimer's disease. A longitudinal MRI study. Brain. 1996;119:2001–2007. - PubMed
-
- Fox NC, Scahill RI, Crum WR, Rossor MN. Correlation between rates of brain atrophy and cognitive decline in AD. Neurology. 1999;52:1687–1689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical