

Lung transplantation and survival in children with cystic fibrosis
- PMID: 18032764
- PMCID: PMC2522236
- DOI: 10.1056/NEJMoa066359
Lung transplantation and survival in children with cystic fibrosis
Erratum in
- N Engl J Med. 2008 Jul 31;359(5):e6
Abstract
Background: The effects of lung transplantation on the survival and quality of life in children with cystic fibrosis are uncertain.
Methods: We used data from the U.S. Cystic Fibrosis Foundation Patient Registry and from the Organ Procurement and Transplantation Network to identify children with cystic fibrosis who were on the waiting list for lung transplantation during the period from 1992 through 2002. We performed proportional-hazards survival modeling, using multiple clinically relevant covariates that were available before the children were on the waiting list and the interactions of these covariates with lung transplantation as a time-dependent covariate. The data were insufficient in quality and quantity for a retrospective quality-of-life analysis.
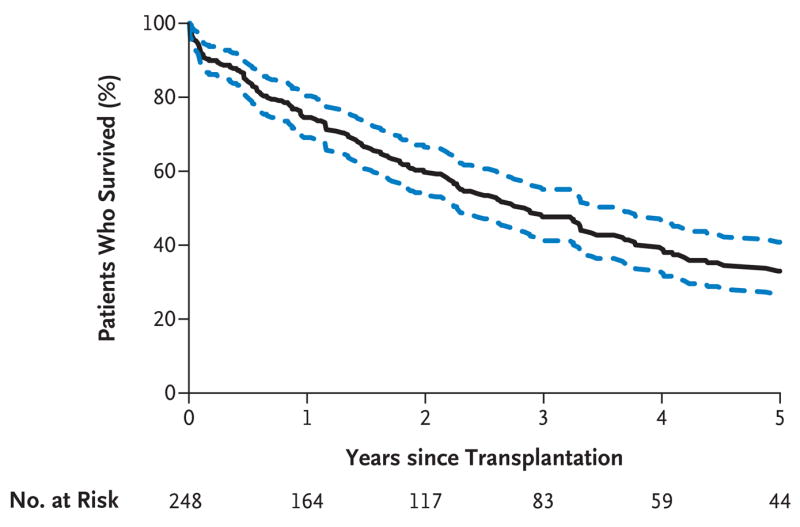
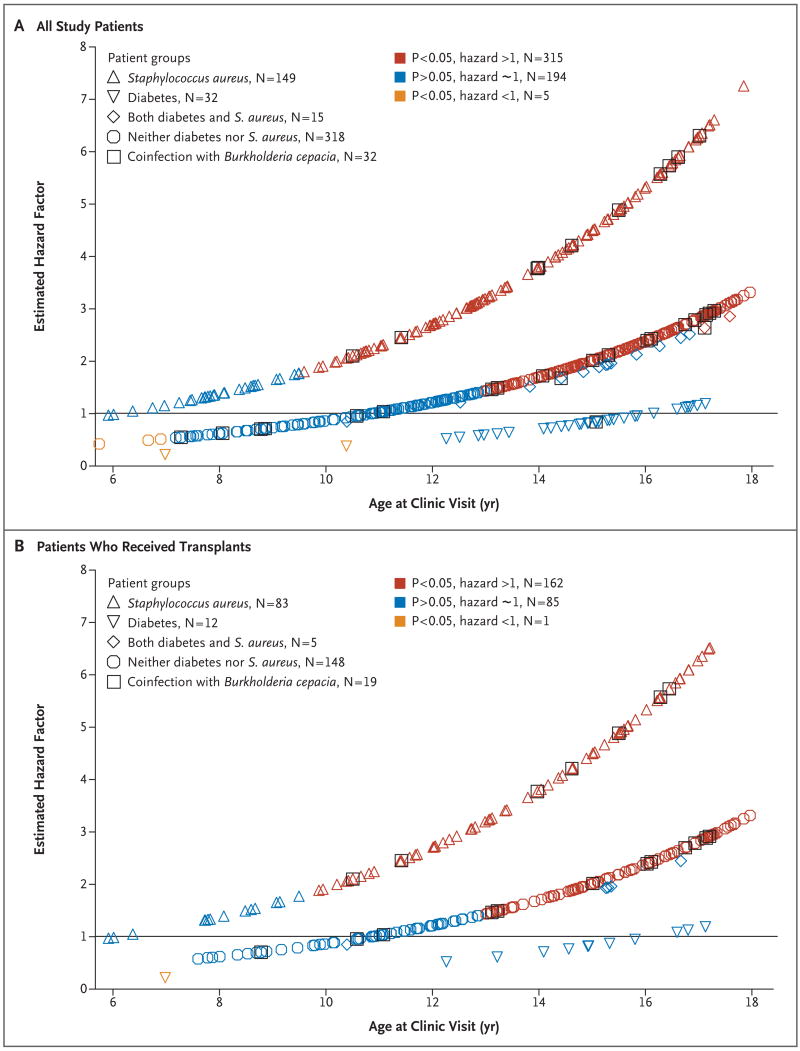
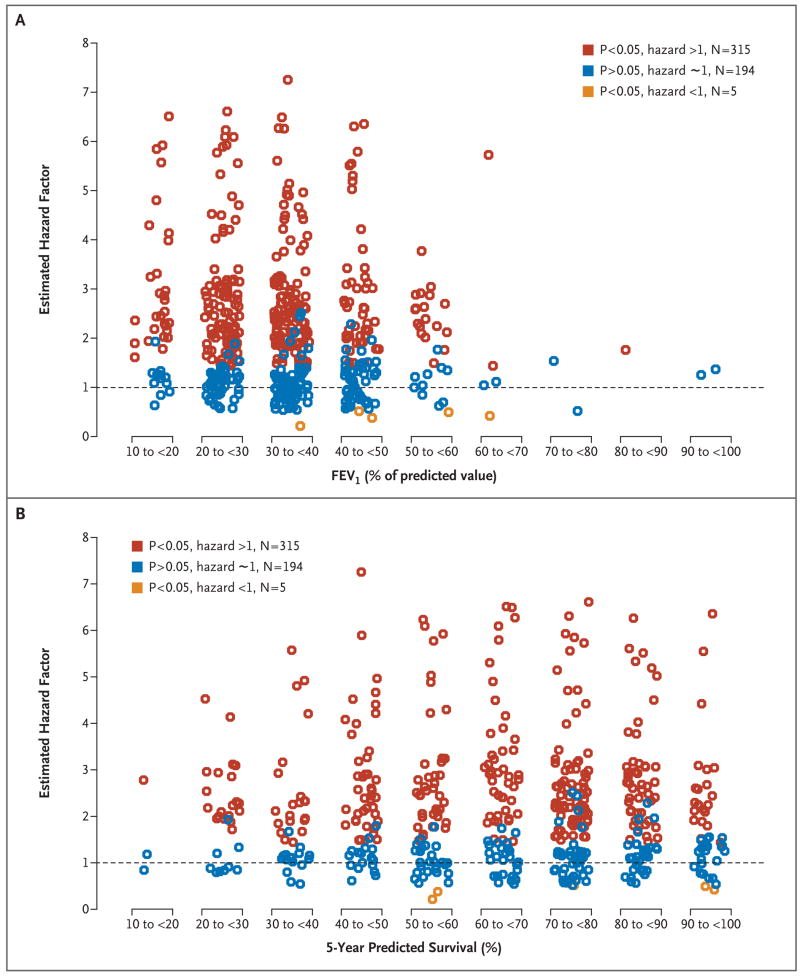
Results: A total of 248 of the 514 children on the waiting list underwent lung transplantation in the United States during the period from 1992 through 2002. Proportional-hazards modeling identified four variables besides transplantation that were associated with changes in survival. Burkholderia cepacia infection was associated with a trend toward decreased survival, regardless of whether the patient underwent transplantation [corrected]. A diagnosis of diabetes before the patient was placed on the waiting list decreased survival while the patient was on the waiting list but did not decrease survival after transplantation, whereas older age did not affect waiting-list survival but decreased post-transplantation survival. Staphylococcus aureus infection increased waiting-list survival but decreased post-transplantation survival. Using age, diabetes status, and S. aureus infection status as covariates, we estimated the effect of transplantation on survival for each patient group, expressed as a hazard factor of less than 1 for a benefit and more than 1 for a risk of harm. Five patients had a significant estimated benefit, 283 patients had a significant risk of harm, 102 patients had an insignificant benefit, and 124 patients had an insignificant risk of harm associated with lung transplantation [corrected].
Conclusions: Our analyses estimated clearly improved survival for only 5 of 514 patients on the waiting list for lung transplantation. Prolongation of life by means of lung transplantation should not be expected in children with cystic fibrosis. A prospective, randomized trial is needed to clarify whether and when patients derive a survival and quality-of-life benefit from lung transplantation.
Copyright 2007 Massachusetts Medical Society.
Figures
Comment in
-
Lung transplantation in cystic fibrosis--primum non nocere?N Engl J Med. 2007 Nov 22;357(21):2186-8. doi: 10.1056/NEJMe078179. N Engl J Med. 2007. PMID: 18032769 No abstract available.
-
Lung transplantation and survival in children with cystic fibrosis.N Engl J Med. 2008 Apr 17;358(16):1753-4; author reply 1755. doi: 10.1056/NEJMc073448. N Engl J Med. 2008. PMID: 18420511 No abstract available.
-
Lung transplantation and survival in children with cystic fibrosis.N Engl J Med. 2008 Apr 17;358(16):1754; author reply 1755. N Engl J Med. 2008. PMID: 18426003 No abstract available.
-
Lung transplantation and survival in children with cystic fibrosis.N Engl J Med. 2008 Apr 17;358(16):1754; author reply 1755. N Engl J Med. 2008. PMID: 18426004 No abstract available.
-
Correction: Lung transplantation and survival in children with cystic fibrosis.N Engl J Med. 2008 Jul 31;359(5):536. doi: 10.1056/NEJMc086289. N Engl J Med. 2008. PMID: 18669438 Free PMC article. No abstract available.
References
-
- Cystic Fibrosis Foundation Patient Registry. 2002 annual data report to the center directors. Bethesda, MD: Cystic Fibrosis Foundation; 2003.
-
- Department of Health and Human Services. Annual report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: transplant data 1995–2004. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation; 2005.
-
- Hosenpud JD, Bennett LE, Keck BM, Edwards EB, Novick RJ. Effect of diagnosis on survival benefit of lung transplantation for end-stage lung disease. Lancet. 1998;351:24–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical