

Vasopressin directly regulates cyst growth in polycystic kidney disease
- PMID: 18032793
- PMCID: PMC2391034
- DOI: 10.1681/ASN.2007060688
Vasopressin directly regulates cyst growth in polycystic kidney disease
Abstract
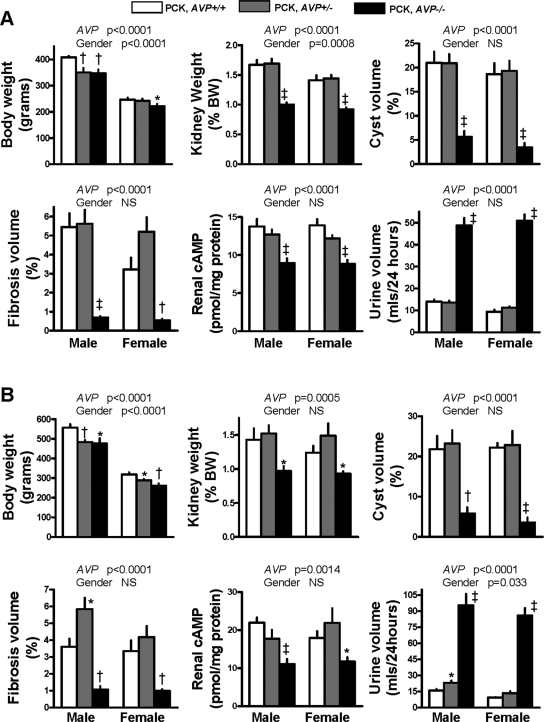
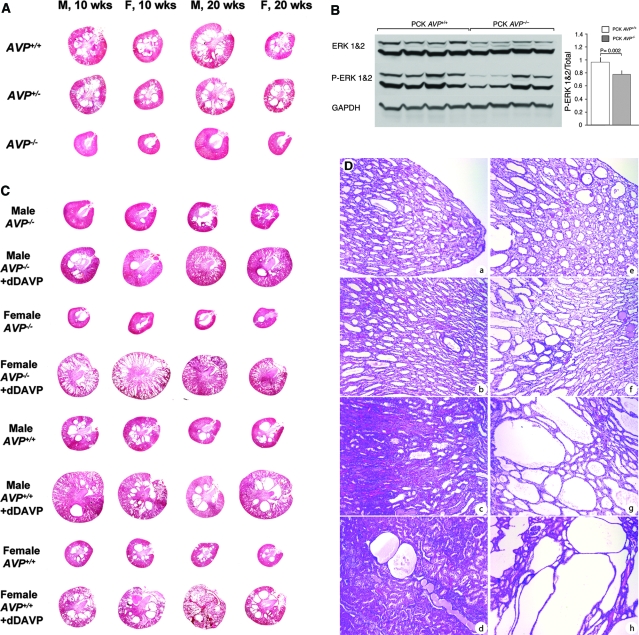
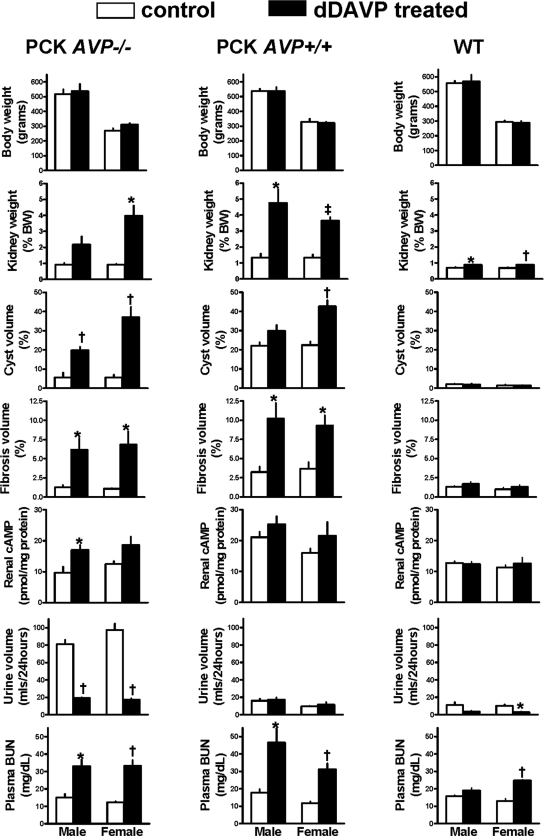
The polycystic kidney diseases (PKD) are a group of genetic disorders causing renal failure and death from infancy to adulthood. Arginine vasopressin (AVP) V2 receptor antagonists inhibit cystogenesis in animal models of cystic kidney diseases, presumably by downregulating cAMP signaling, cell proliferation, and chloride-driven fluid secretion. For confirmation that the protective effect of these drugs is due to antagonism of AVP, PCK (Pkhd1(-/-)) and Brattleboro (AVP(-/-)) rats were crossed to generate rats with PKD and varying amounts of AVP. At 10 and 20 weeks of age, PCK AVP(-/-) rats had lower renal cAMP and almost complete inhibition of cystogenesis compared with PCK AVP(+/+) and PCK AVP(+/-) rats. The V2 receptor agonist 1-deamino-8-d-arginine vasopressin increased renal cAMP and recovered the full cystic phenotype of PCK AVP(-/-) rats and aggravated the cystic disease of PCK AVP(+/+) rats but did not induce cystic changes in wild-type rats. These observations indicate that AVP is a powerful modulator of cystogenesis and provide further support for clinical trials of V2 receptor antagonists in PKD.
Figures
Comment in
-
Therapy for polycystic kidney disease? It's water, stupid!J Am Soc Nephrol. 2008 Jan;19(1):1-7. doi: 10.1681/ASN.2007101100. Epub 2007 Nov 21. J Am Soc Nephrol. 2008. PMID: 18032792 No abstract available.
References
-
- Torres VE, Harris PC, Pirson Y: Autosomal dominant polycystic kidney disease. Lancet 369: 1287–1301, 2007 - PubMed
-
- Torres VE, Harris PC: Mechanisms of disease: Autosomal dominant and recessive polycystic kidney diseases. Nat Clin Pract Nephrol 2: 40–54, 2006 - PubMed
-
- Gattone VH, Wang X, Harris PC, Torres VE: Inhibition of renal cystic disease development and progression by a vasopressin V2 receptor antagonist. Nat Med 9: 1323–1326, 2003 - PubMed
-
- Torres VE, Wang X, Qian Q, Somlo S, Harris PC, Gattone VH: Effective treatment of an orthologous model of autosomal dominant polycystic kidney disease. Nat Med 10: 363–364, 2004 - PubMed
-
- Wang X, Gattone VH II, Harris PC, Torres VE: Effectiveness of vasopressin V2 receptor antagonists OPC-31260 and OPC-41061 on polycystic kidney disease development in the PCK rat. J Am Soc Nephrol 16: 846–851, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
