

Noninvasive differentiation of uric acid versus non-uric acid kidney stones using dual-energy CT
- PMID: 18035274
- PMCID: PMC2743375
- DOI: 10.1016/j.acra.2007.09.016
Noninvasive differentiation of uric acid versus non-uric acid kidney stones using dual-energy CT
Abstract
Rationale and objectives: To determine the accuracy and sensitivity for dual-energy computed tomography (DECT) discrimination of uric acid (UA) stones from other (non-UA) renal stones in a commercially implemented product.
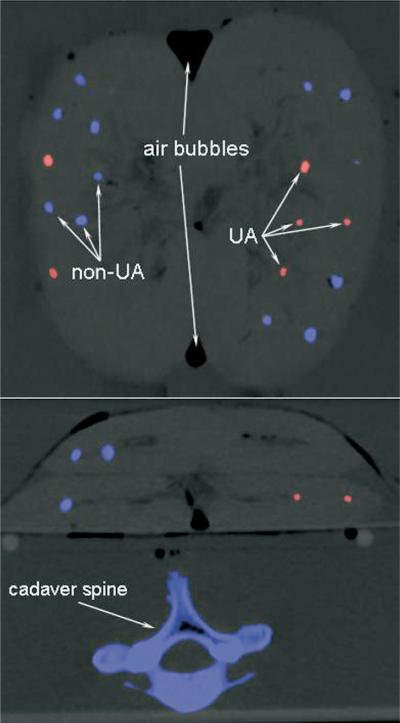
Materials and methods: Forty human renal stones comprising uric acid (n=16), hydroxyapatite (n=8), calcium oxalate (n=8), and cystine (n=8) were inserted in four porcine kidneys (10 each) and placed inside a 32-cm water tank anterior to a cadaver spine. Spiral dual-energy scans were obtained on a dual-source, 64-slice computed tomography (CT) system using a clinical protocol and automatic exposure control. Scanning was performed at two different collimations (0.6 mm and 1.2 mm) and within three phantom sizes (medium, large, and extra large) resulting in a total of six image datasets. These datasets were analyzed using the dual-energy software tool available on the CT system for both accuracy (number of stones correctly classified as either UA or non-UA) and sensitivity (for UA stones). Stone characterization was correlated with micro-CT.
Results: For the medium and large phantom sizes, the DECT technique demonstrated 100% accuracy (40/40), regardless of collimation. For the extra large phantom size and the 0.6-mm collimation (resulting in the noisiest dataset), three (two cystine and one small UA) stones could not be classified (93% accuracy and 94% sensitivity). For the extra large phantom size and the 1.2-mm collimation, the dual-energy tool failed to identify two small UA stones (95% accuracy and 88% sensitivity).
Conclusions: In an anthropomorphic phantom model, dual-energy CT can accurately discriminate uric acid stones from other stone types.
Figures



References
-
- Kawashima A, Vrtiska TJ, LeRoy AJ, et al. CT urography. Radiographics. 2004;24(Suppl 1):S35–S58. - PubMed
-
- Kalra MK, Maher MM, D'Souza RV, et al. Detection of urinary tract stones at low-radiation-dose CT with z-axis automatic tube current modulation: phantom and clinical studies. Radiology. 2005;235:523–529. - PubMed
-
- Heneghan JP, McGuire KA, Leder RA, et al. Helical CT for nephrolithiasis and ureterolithiasis: comparison of conventional and reduced radiation-dose techniques. Radiology. 2003;229:575–580. - PubMed
-
- Williams JC, Jr, Kim SC, Zarse CA, et al. Progress in the use of helical CT for imaging urinary calculi. J Endourol. 2004;18:937–941. - PubMed
-
- Vrtiska TJ. Quantitation of stone burden: imaging advances. Urol Res. 2005:33398–402. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
