

Relationships of N-terminal pro-B-natriuretic peptide and cardiac troponin T to left ventricular mass and function and mortality in asymptomatic hemodialysis patients
- PMID: 18037101
- PMCID: PMC2408379
- DOI: 10.1053/j.ajkd.2007.08.017
Relationships of N-terminal pro-B-natriuretic peptide and cardiac troponin T to left ventricular mass and function and mortality in asymptomatic hemodialysis patients
Abstract
Background: Although the cardiac biomarker troponin T (cTnT) is related strongly to mortality in patients with end-stage renal disease, the independent association of N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) and cTnT levels in predicting outcomes is unknown. The objective of this study is to determine factors associated with NT-pro-BNP and cTnT and determine whether these levels are associated with mortality.
Study design: Cohort study.
Setting & participants: Asymptomatic hemodialysis patients (n = 150) in 4 university-affiliated hemodialysis units. EXPOSURE & OUTCOMES: For cross-sectional analysis, echocardiographic variables as exposures and NT-pro-BNP and cTnT levels as outcomes; for longitudinal analysis, association of NT-pro-BNP and cTnT levels as exposures to all-cause and cardiovascular disease mortality as outcomes.
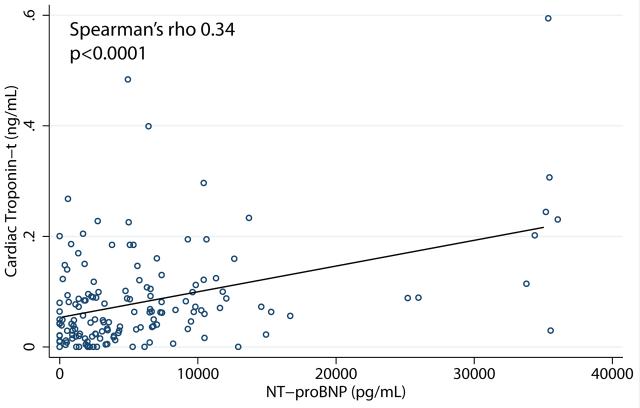
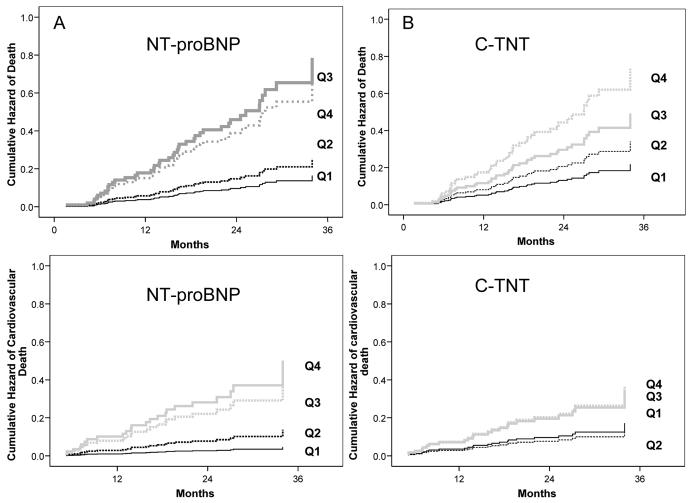
Results: In a multivariate regression analysis, low midwall fractional shortening, a measure of poor systolic function, was an independent correlate of log NT-pro-BNP level (P < 0.01), whereas left ventricular mass index was an independent correlate of cTnT level (P < 0.01). During a median follow-up of 24 months, 46 patients died, 26 of cardiovascular causes. NT-pro-BNP levels had a strong graded relationship with all-cause (hazard ratios [HRs], 1.54, 4.78, and 4.03 for increasing quartiles; P < 0.001) and cardiovascular mortality (HRs, 2.99, 10.95, and 8.54; P < 0.01), whereas cTnT level had a weaker relationship with all-cause (HRs, 1.57, 2.32, and 3.39; P < 0.01) and cardiovascular mortality (HRs, 0.81, 2.12, and 2.14; P = 0.1). The combination of the 2 biomarker levels did not improve the association with all-cause or cardiovascular mortality compared with NT-pro-BNP level alone. NT-pro-BNP level was a marker of mortality even after adjusting for left ventricular mass index and midwall fractional shortening.
Limitations: Our cohort was predominantly black and of limited sample size.
Conclusion: NT-pro-BNP level strongly correlates with left ventricular systolic dysfunction and is associated more strongly with mortality than cTnT level in asymptomatic hemodialysis patients.
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, et al. The prognostic importance of left ventricular geometry in uremic cardiomyopathy. J Am Soc Nephrol. 1995;5:2024–2031. - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, et al. Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Kidney Int. 1995;47:186–192. - PubMed
-
- Roberts MA, Hare DL, Ratnaike S, et al. Cardiovascular biomarkers in CKD: pathophysiology and implications for clinical management of cardiac disease. Am J Kidney Dis. 2006;48:341–360. - PubMed
-
- Iliou MC, Fumeron C, Benoit MO, et al. Prognostic value of cardiac markers in ESRD: Chronic Hemodialysis and New Cardiac Markers Evaluation (CHANCE) study. Am J Kidney Dis. 2003;42:513–523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
