

Review
doi: 10.1016/j.rdc.2007.08.002.
Scleritis and peripheral ulcerative keratitis
Affiliations
- PMID: 18037120
- PMCID: PMC2212596
- DOI: 10.1016/j.rdc.2007.08.002
Item in Clipboard
Review
Scleritis and peripheral ulcerative keratitis
Rheum Dis Clin North Am.
2007 Nov.
Abstract
Scleritis and peripheral ulcerative keratitis (PUK) can present as isolated conditions or as part of a systemic inflammatory or infectious disorder. Both are serious ocular conditions that can result in vision loss and require early diagnosis and treatment. Nearly two thirds of patients with non-infectious scleritis require systemic glucocorticoid therapy and one fourth need a glucocorticoid-sparing agent as well. Essentially all patients with non-infectious PUK require systemic glucocorticoids. A detailed clinical history, thorough physical examination, and thoughtful laboratory evaluations are important in the exclusion of underlying disorders and extraocular involvement.
Figures

Anatomy of the eye
Diffuse anterior scleritis. In addition to the bright red episcleral vessels, there is a deep violaceous hue to the sclera that indicates scleral inflammation.
Active (left) and resolved (right) diffuse anterior scleritis. Resolution of diffuse anterior scleritis in a 50 year-old man with Wegener’s granulomatosis after treatment with prednisone and cyclophosphamide. Resolution of the scleral inflammation has left a bluish gray hue that represents rearrangement of the collagen fibers in the sclera.

Active (left) and resolved (right) diffuse anterior scleritis. Resolution of diffuse anterior scleritis in a 50 year-old man with Wegener’s granulomatosis after treatment with prednisone and cyclophosphamide. Resolution of the scleral inflammation has left a bluish gray hue that represents rearrangement of the collagen fibers in the sclera.

Nodular anterior scleritis. Nodular anterior scleritis in a 44 year-old man with hepatitis C. Along with areas of diffuse scleral inflammation, a discrete, raised, scleral nodule is seen near the limbus at the 5 o’clock position.

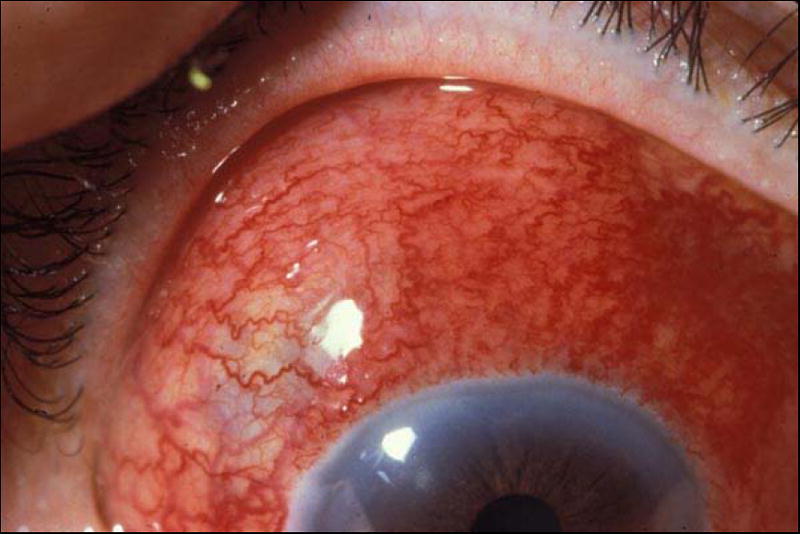
Necrotizing anterior scleritis. Necrotizing anterior scleritis in a 49 year-old woman with hepatitis C associated cryoglobulinemia. Along with nasal episcleral and scleral inflammation, there is an area of scleral whitening that represents an area of necrosis.

Resolved necrotizing anterior scleritis. Resolution of idiopathic necrotizing scleritis in a 36 year-old women after treatment with prednisone and mycophenolate mofetil. The sclera is thin and translucent in the area of previous necrotizing inflammation. The choroidal hue can be appreciated through this area.

Necrotizing anterior scleritis without inflammation (scleromalacia perforans). The patient presented with scleral necrosis and minimal pain. The bluish scleral hue is created by the transmission of choroidal pigment through the thin sclera.

B-scan ultrasonography of posterior scleritis. Idiopathic posterior scleritis in a 51 year-old woman. The figure demonstrates thickened sclera with hypoechogenic fluid in the space behind the sclera.

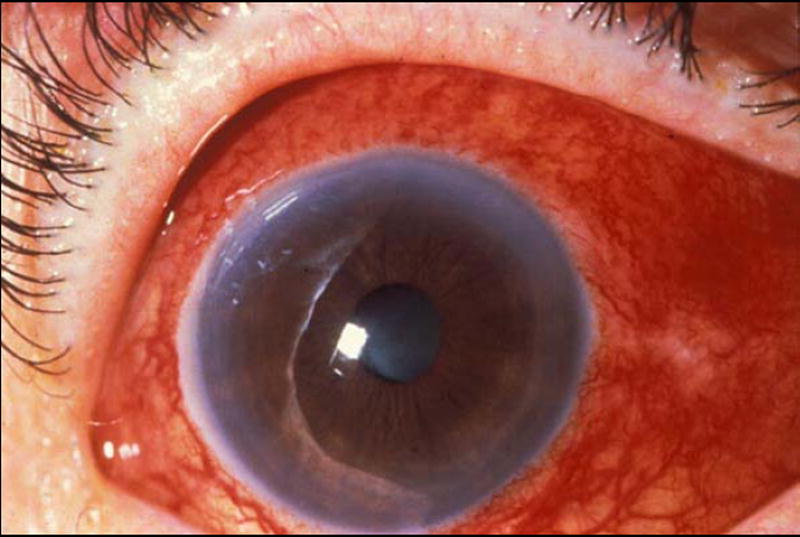
Peripheral ulcerative keratitis. Idiopathic peripheral ulcerative keratitis in a 43 year-old man. A crescent-shaped corneal ulcer with minimal discharge is seen at the nasal limbus.
References
-
- Okhravi N, Odufuwa B, McCluskey P, Lightman S. Scleritis. Surv Ophthalmol. 2005;50(4):351–63. - PubMed
-
- McCluskey PJ, Watson PG, Lightman S, Haybittle J, Restori M, Branley M. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology. 1999;106(12):2380–6. - PubMed
-
- Jabs DA, Mudun A, Dunn JP, Marsh MJ. Episcleritis and scleritis: clinical features and treatment results. Am J Ophthalmol. 2000;130(4):469–76. - PubMed
-
- Joysey VC, Roger JH, Ashworth F, et al. Parallel studies of HLA antigens in patients with rheumatic heart disease and scleritis: comparisons with three control populations. J Rheumatol Suppl. 1977;3:84–8. - PubMed
-
- Smith JR, Mackensen F, Rosenbaum JT. Therapy insight: scleritis and its relationship to systemic autoimmune disease. Nat Clin Pract Rheumatol. 2007;3(4):219–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
