

A T1 hyperintense perilesional signal aids in the differentiation of a cavernous angioma from other hemorrhagic masses
- PMID: 18039756
- PMCID: PMC8118872
- DOI: 10.3174/ajnr.A0847
A T1 hyperintense perilesional signal aids in the differentiation of a cavernous angioma from other hemorrhagic masses
Abstract
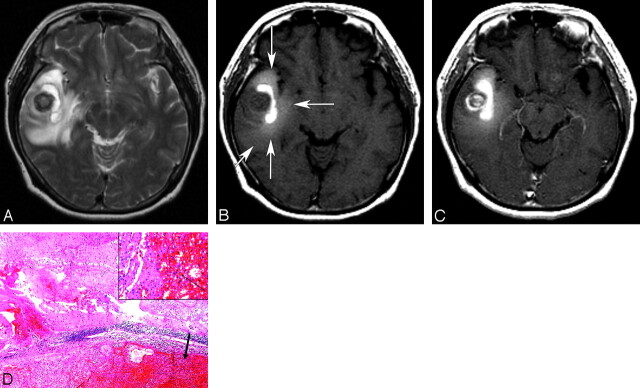
Background and purpose: A cavernous angioma is a developmental vascular malformation with a high risk of hemorrhage. The purpose of this work was to retrospectively determine whether an MR sign of T1 hyperintense perilesional signal intensity is useful for the differentiation of cavernous angioma from other hemorrhagic cerebral masses.
Materials and methods: The institutional review board approved this study. We retrospectively evaluated the MR images of 72 patients with acute or subacute cerebral hemorrhagic lesions with perilesional edema (29 cavernous angiomas, 13 glioblastomas, 1 oligodendroglioma, 16 metastatic tumors, and 13 intracerebral hemorrhages) for the presence of T1 hyperintense perilesional signal intensity. In addition, T1 signal intensities of a perilesional edema were quantitatively analyzed. In cavernous angiomas, volumes of hemorrhagic lesions and perilesional edemas, lesion locations, presence of contrast enhancement, and time intervals between symptom onset and MR imaging were also assessed. Data were analyzed using unpaired t test or Fisher exact test.
Results: T1 hyperintense perilesional signal intensity sign was found in 18 (62.1%) of 29 cavernous angiomas, in 1 (6.3%) of 16 metastases, and in 0 primary brain tumors or intracerebral hemorrhages. Sensitivity, specificity, and positive predictive value of this sign for cavernous angioma were 62%, 98%, and 95%, respectively. The perilesional T1 hyperintensity was significantly higher in cavernous angiomas (P = .045) than in normal white matter. Perilesional edema volumes were larger in cavernous angiomas with the MR sign than in cavernous angiomas without the sign (P = .009).
Conclusion: When the MR sign of T1 hyperintense perilesional signal intensity is present, there is a high probability of cavernous angioma being present in the brain, and this MR sign may be helpful for differentiating cavernous angioma from hemorrhagic tumors and intracerebral hemorrhages.
Figures
References
-
- Zabramski JM, Wascher TM, Spetzler RF, et al. The natural history of familial cavernous malformations: results of an ongoing study. J Neurosurg 1994;80:422–32 - PubMed
-
- Rigamonti D, Drayer BP, Johnson PC, et al. The MRI appearance of cavernous malformations (angiomas). J Neurosurg 1987;67:518–24 - PubMed
-
- Dorsch NWC, McMahon JHA. Intracranial cavernous malformations—natural history and management. Crit Rev Neurosurg 1998;8:154–68 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical