

Temporal trends and predictors of perioperative chemotherapy use in elderly patients with resected nonsmall cell lung cancer
- PMID: 18041068
- PMCID: PMC3768264
- DOI: 10.1002/cncr.23181
Temporal trends and predictors of perioperative chemotherapy use in elderly patients with resected nonsmall cell lung cancer
Abstract
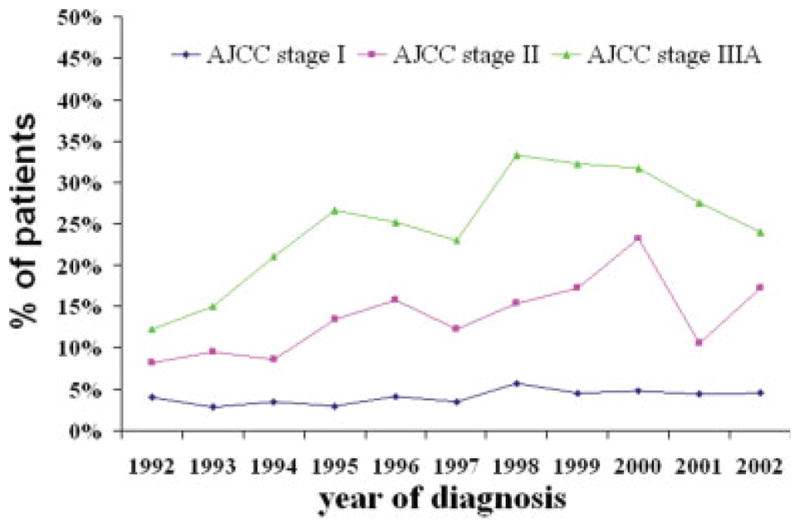
Background: The authors assessed patterns of perioperative chemotherapy use in elderly patients with resected stage I, II, or IIIA nonsmall cell lung cancer (NSCLC) from 1992 to 2002.
Methods: By using data from the Surveillance, Epidemiology, and End Results Program, 11,807 patients were identified who had resected stage I, II, or IIIA NSCLC between 1992 and 2002 and survived >or=120 days beyond diagnosis. The rate of perioperative chemotherapy use was measured by calendar year, and the association between clinical/demographic characteristics and the receipt of chemotherapy was examined by using logistic regression.
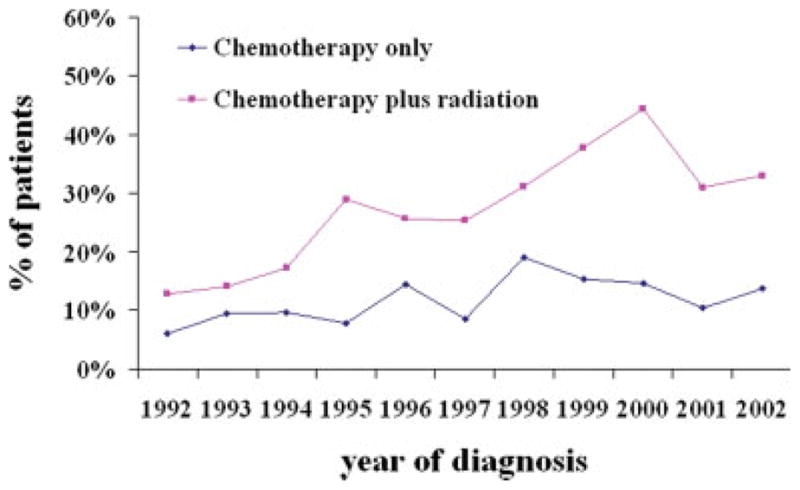
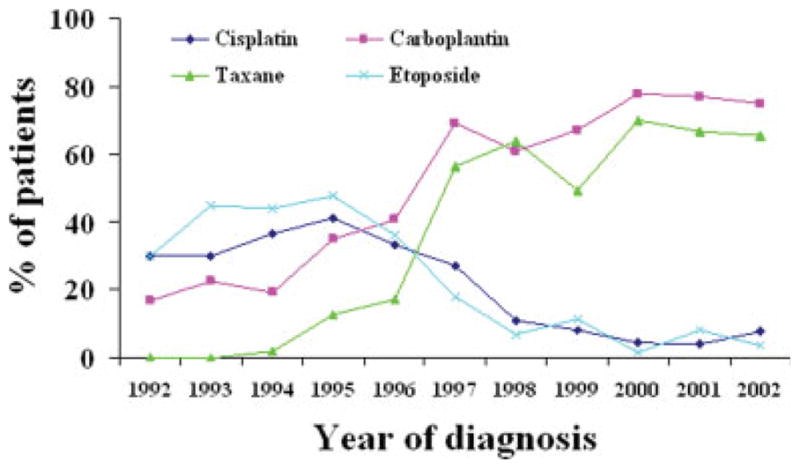
Results: In total, 957 patients with stage I, II, or IIIA NSCLC (8.1% of the study population) received perioperative chemotherapy. The proportion of patients receiving chemotherapy for stage I NSCLC changed little during the study period. Of 3230 patients with stage II and IIIA NSCLC, 609 patients (18.9%) received chemotherapy, 423 patients (13%) received chemotherapy combined with radiation. 452 patients (15.6%) received adjuvant chemotherapy, and 66 patients (2.3%) received neoadjuvant chemotherapy. The use of chemotherapy increased significantly among patients who were diagnosed after 1994 relative to patients who were diagnosed in 1992 after controlling for sociodemographic and treatment characteristics (P< .001). There was significantly increased use of new-generation chemotherapy agents, such as carboplatin and taxanes (P< .001). The proportion of patients receiving combined-modality therapy also increased significant (P< .001). Younger age, being married, having advanced-stage tumor or adenocarcinoma, having a later diagnosis year, receiving radiation, and seeing an oncologist were predictors for the receipt of chemotherapy (P< .001).
Conclusions: A substantial proportion of Medicare beneficiaries with NSCLC received perioperative chemotherapy. Specifically designed prospective trials that focus on older patients are needed.
Figures
Similar articles
-
Treatment Patterns and Outcomes in Resected Early-stage Non-small Cell Lung Cancer: An Analysis of the SEER-Medicare Data.Clin Lung Cancer. 2023 May;24(3):260-268. doi: 10.1016/j.cllc.2022.12.005. Epub 2022 Dec 25. Clin Lung Cancer. 2023. PMID: 36641325
-
Increasing access to medical oncology consultation in older patients with stage II-IIIA non-small-cell lung cancer.Med Oncol. 2008;25(2):125-32. doi: 10.1007/s12032-007-9003-5. Epub 2007 Sep 5. Med Oncol. 2008. PMID: 18488153 Free PMC article.
-
Adjuvant chemotherapy for elderly patients with stage I non-small-cell lung cancer ≥4 cm in size: an SEER-Medicare analysis.Ann Oncol. 2015 Apr;26(4):768-773. doi: 10.1093/annonc/mdv008. Epub 2015 Jan 18. Ann Oncol. 2015. PMID: 25600562
-
The present status of postoperative adjuvant chemotherapy for completely resected non-small cell lung cancer.Ann Thorac Cardiovasc Surg. 2007 Apr;13(2):73-7. Ann Thorac Cardiovasc Surg. 2007. PMID: 17505412 Review.
-
Clinical issues in the management of non-small-cell lung cancer and the role of platinum-based therapy.Clin Lung Cancer. 2004 Mar;5(5):274-89. doi: 10.3816/CLC.2004.n.007. Clin Lung Cancer. 2004. PMID: 15086966 Review.
Cited by
-
Institutional factors associated with adherence to quality measures for stage I and II non-small cell lung cancer.J Thorac Cardiovasc Surg. 2021 Sep;162(3):649-660.e8. doi: 10.1016/j.jtcvs.2020.05.123. Epub 2020 Jul 29. J Thorac Cardiovasc Surg. 2021. PMID: 34144822 Free PMC article.
-
Lung cancer treatment costs, including patient responsibility, by disease stage and treatment modality, 1992 to 2003.Value Health. 2011 Jan;14(1):41-52. doi: 10.1016/j.jval.2010.10.006. Value Health. 2011. PMID: 21211485 Free PMC article.
-
NSCLC in the elderly--the legacy of therapeutic neglect.Curr Treat Options Oncol. 2009 Aug;10(3-4):180-94. doi: 10.1007/s11864-009-0099-z. Epub 2009 May 16. Curr Treat Options Oncol. 2009. PMID: 19449105 Review.
-
Identifying specific chemotherapeutic agents in Medicare data: a validation study.Med Care. 2013 May;51(5):e27-34. doi: 10.1097/MLR.0b013e31823ab60f. Med Care. 2013. PMID: 22080337 Free PMC article.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, Thun MJ. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–130. - PubMed
-
- Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2:533–543. - PubMed
-
- Spira A, Ettinger DS. Multidisciplinary management of lung cancer. N Engl J Med. 2004;350:379–392. - PubMed
-
- Immerman SC, Vanecko RM, Fry WA, Head LR, Shields TW. Site of recurrence in patients with stages I and II carcinoma of the lung resected for cure. Ann Thorac Surg. 1981;32:23–27. - PubMed
-
- Rosell R, Felip E, Maestre J, et al. The role of chemotherapy in early non-small-cell lung cancer management. Lung Cancer. 2001;34(suppl 3):S63–S74. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
