

Sonographic measurement of lateral parapharyngeal wall thickness in patients with obstructive sleep apnea
- PMID: 18041482
- PMCID: PMC2082100
- DOI: 10.1093/sleep/30.11.1503
Sonographic measurement of lateral parapharyngeal wall thickness in patients with obstructive sleep apnea
Abstract
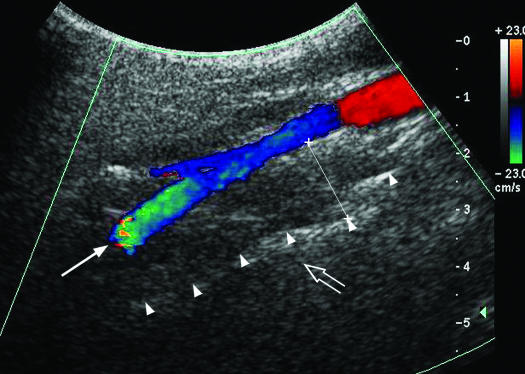
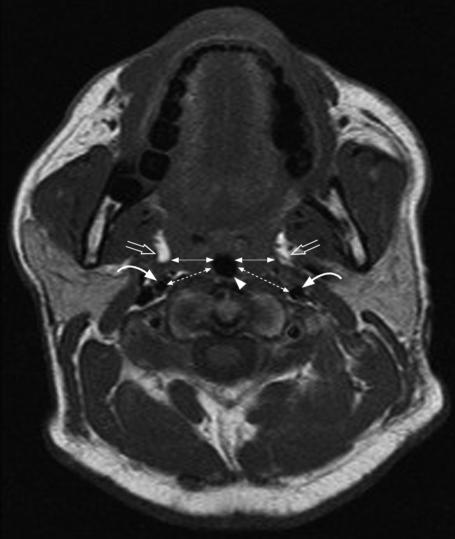
Introduction: Lateral parapharyngeal wall (LPW) thickness may be a predominant anatomic factor causing airway narrowing in apneic subjects. In this study, we explored sonographic measurement of the LPW thickness and compared the results with LPW thickness measured by magnetic resonance imaging (MRI). We also investigated the association between sonographic measurement of LPW thickness and apnea-hypopnea index (AHI).
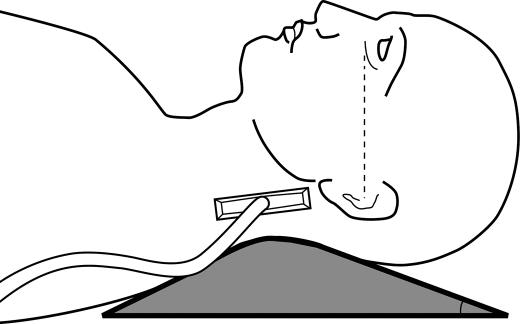
Method: Seventy-six patients with suspected obstructive sleep apnea (OSA) underwent ultrasound examination of LPW thickness after overnight polysomnography. Fifteen out of 76 subjects also participated in correlation and reliability studies of sonographic and MRI measurements of LPW thickness.
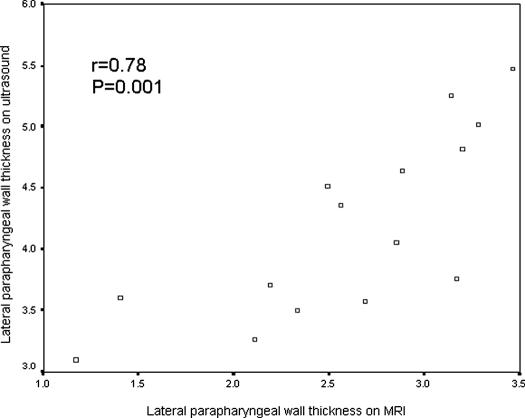
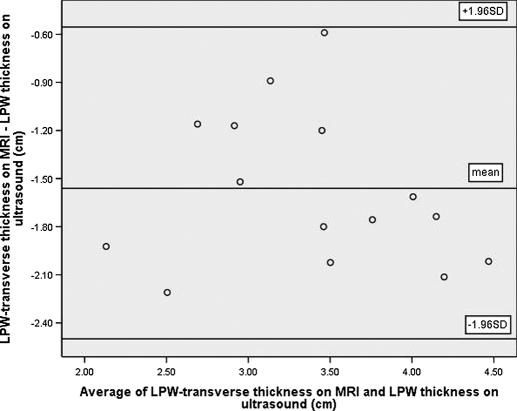
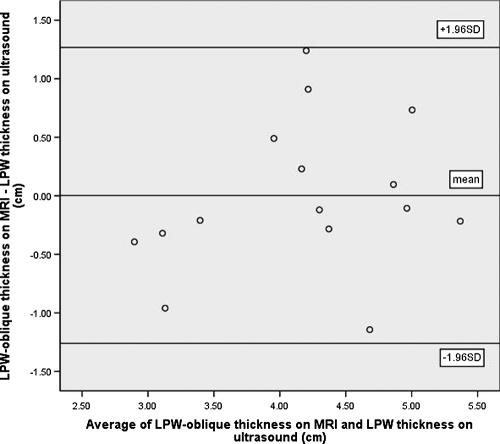
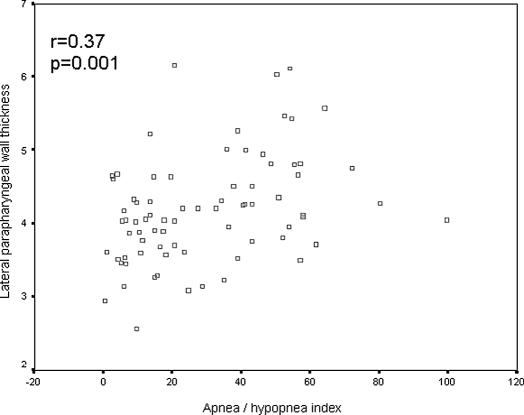
Results: There was good correlation between measurements of LPW thickness on ultrasound and MRI (r = 0.78, P = 0.001), although Bland-Altman analysis indicated overestimation of LPW thickness by ultrasound, when compared with the LPW as measured by MRI. The sonographic measurement of LPW thickness had high reproducibility, with intraclass correlation coefficients of 0.90 and 0.97 for intraoperator and interoperator reliability, respectively. Fifty-eight subjects with significant OSA (AHI > or = 10/h) had a higher body mass index, larger neck circumference, and greater LPW thickness measured by ultrasound than those (n = 18) with an AHI of less than 10 per hour. LPW thickness had a positive correlation with AHI on univariate analysis (r = 0.37, P = 0.001). On multivariate analysis, LPW thickness had a positive independent association with AHI after adjustment for age, sex, neck circumference, and body mass index. The positive association of LPW thickness with AHI remained significant in both univariate and multivariate analyses of men only (n = 62).
Conclusions: Sonographic measurement of LPW thickness is a novel and reliable technique and had good correlations with measurement by MRI and the severity of OSA. Ultrasound may provide an alternative imaging modality with easy accessibility and lower cost in OSA research.
Figures
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;329:1230–5. - PubMed
-
- Ip MS, Lam B, Lauder IJ, et al. A community study of sleep-disordered breathing in middle-aged Chinese men in Hong Kong. Chest. 2001;119:62–9. - PubMed
-
- Hui DS, Ko FW, Chan JK, et al. Sleep disordered breathing and CPAP compliance in a group of commercial bus drivers in Hong Kong. Respirology. 2006;11:723–30. - PubMed
-
- White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med. 2005;172:1363–70. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
