

Acromioclavicular joint dislocation: a comparative biomechanical study of the palmaris-longus tendon graft reconstruction with other augmentative methods in cadaveric models
- PMID: 18042292
- PMCID: PMC2235831
- DOI: 10.1186/1749-799X-2-22
Acromioclavicular joint dislocation: a comparative biomechanical study of the palmaris-longus tendon graft reconstruction with other augmentative methods in cadaveric models
Abstract
Background: Acromioclavicular injuries are common in sports medicine. Surgical intervention is generally advocated for chronic instability of Rockwood grade III and more severe injuries. Various methods of coracoclavicular ligament reconstruction and augmentation have been described. The objective of this study is to compare the biomechanical properties of a novel palmaris-longus tendon reconstruction with those of the native AC+CC ligaments, the modified Weaver-Dunn reconstruction, the ACJ capsuloligamentous complex repair, screw and clavicle hook plate augmentation.
Hypothesis: There is no difference, biomechanically, amongst the various reconstruction and augmentative methods.
Study design: Controlled laboratory cadaveric study.
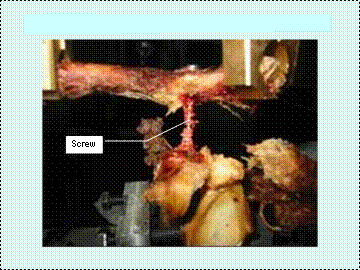
Methods: 54 cadaveric native (acromioclavicular and coracoclavicular) ligaments were tested using the Instron machine. Superior loading was performed in the 6 groups: 1) in the intact states, 2) after modified Weaver-Dunn reconstruction (WD), 3) after modified Weaver-Dunn reconstruction with acromioclavicular joint capsuloligamentous repair (WD.ACJ), 4) after modified Weaver-Dunn reconstruction with clavicular hook plate augmentation (WD.CP) or 5) after modified Weaver-Dunn reconstruction with coracoclavicular screw augmentation (WD.BS) and 6) after modified Weaver-Dunn reconstruction with mersilene tape-palmaris-longus tendon graft reconstruction (WD. PLmt). Posterior-anterior (horizontal) loading was similarly performed in all groups, except groups 4 and 5. The respective failure loads, stiffnesses, displacements at failure and modes of failure were recorded. Data analysis was carried out using a one-way ANOVA, with Student's unpaired t-test for unpaired data (S-PLUS statistical package 2005).
Results: Native ligaments were the strongest and stiffest when compared to other modes of reconstruction and augmentation except coracoclavicular screw, in both posterior-anterior and superior directions (p < 0.005).WD.ACJ provided additional posterior-anterior (P = 0. 039) but not superior (p = 0.250) stability when compared to WD alone.WD+PLmt, in loads and stiffness at failure superiorly, was similar to WD+CP (p = 0.066). WD+PLmt, in loads and stiffness at failure postero-anteriorly, was similar to WD+ACJ (p = 0.084).Superiorly, WD+CP had similar strength as WD+BS (p = 0.057), but it was less stiff (p < 0.005).
Conclusions and clinical relevance: Modified Weaver-Dunn procedure must always be supplemented with acromioclavicular capsuloligamentous repair to increase posterior-anterior stability. Palmaris-Longus tendon graft provides both additional superior and posterior-anterior stability when used for acromioclavicular capsuloligamentous reconstruction. It is a good alternative to clavicle hook plate in acromioclavicular dislocation.
Figures




References
-
- Bargren JH, Erlanger S, Dick HM. Biomechanics and comparison of two operative methods of treatment of complete acromioclavicular separation. Clin Orthop. 1978;130:267–272. - PubMed
-
- Bosworth BM. Acromioclavicular separation. A new method of repair. Surg Gynecol Obstet. 1941;73:866–871.
-
- Cadenat FM. The treatment of dislocations and fractures of the outer end of the clavicle. Int Clin. 1917;27:145–69.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
