

Importance of baseline prognostic factors with increasing time since initiation of highly active antiretroviral therapy: collaborative analysis of cohorts of HIV-1-infected patients
- PMID: 18043315
- PMCID: PMC3687569
- DOI: 10.1097/QAI.0b013e31815b7dba
Importance of baseline prognostic factors with increasing time since initiation of highly active antiretroviral therapy: collaborative analysis of cohorts of HIV-1-infected patients
Abstract
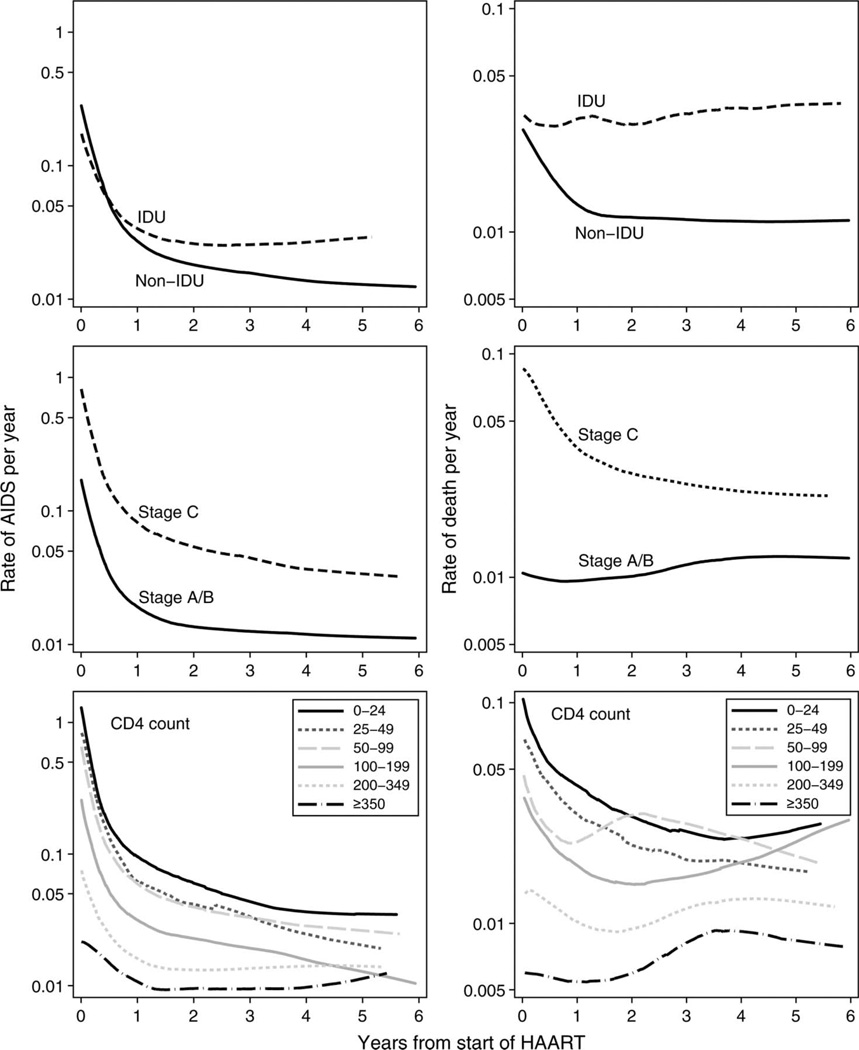
Background: The extent to which the prognosis for AIDS and death of patients initiating highly active antiretroviral therapy (HAART) continues to be affected by their characteristics at the time of initiation (baseline) is unclear.
Methods: We analyzed data on 20,379 treatment-naive HIV-1-infected adults who started HAART in 1 of 12 cohort studies in Europe and North America (61,798 person-years of follow-up, 1844 AIDS events, and 1005 deaths).
Results: Although baseline CD4 cell count became less prognostic with time, individuals with a baseline CD4 count <25 cells/microL had persistently higher progression rates than individuals with a baseline CD4 count >350 cells/microL (hazard ratio for AIDS = 2.3, 95% confidence interval [CI]: 1.0 to 2.3; mortality hazard ratio = 2.5, 95% CI: 1.2 to 5.5, 4 to 6 years after starting HAART). Rates of AIDS were persistently higher in individuals who had experienced an AIDS event before starting HAART. Individuals with presumed transmission by means of injection drug use experienced substantially higher rates of AIDS and death than other individuals throughout follow-up (AIDS hazard ratio = 1.6, 95% CI: 0.8 to 3.0; mortality hazard ratio = 3.5, 95% CI: 2.2 to 5.5, 4 to 6 years after starting HAART).
Conclusions: Compared with other patient groups, injection drug users and patients with advanced immunodeficiency at baseline experience substantially increased rates of AIDS and death up to 6 years after starting HAART.
Figures
Similar articles
-
Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies.Lancet. 2002 Jul 13;360(9327):119-29. doi: 10.1016/s0140-6736(02)09411-4. Lancet. 2002. PMID: 12126821
-
Prognostic importance of initial response in HIV-1 infected patients starting potent antiretroviral therapy: analysis of prospective studies.Lancet. 2003 Aug 30;362(9385):679-86. doi: 10.1016/s0140-6736(03)14229-8. Lancet. 2003. PMID: 12957089
-
Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies.Lancet. 2009 Apr 18;373(9672):1352-63. doi: 10.1016/S0140-6736(09)60612-7. Epub 2009 Apr 8. Lancet. 2009. PMID: 19361855 Free PMC article. Review.
-
Causes of death in HIV-1-infected patients treated with antiretroviral therapy, 1996-2006: collaborative analysis of 13 HIV cohort studies.Clin Infect Dis. 2010 May 15;50(10):1387-96. doi: 10.1086/652283. Clin Infect Dis. 2010. PMID: 20380565 Free PMC article.
-
HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis.Lancet. 2006 Aug 5;368(9534):451-8. doi: 10.1016/S0140-6736(06)69152-6. Lancet. 2006. PMID: 16890831 Review.
Cited by
-
Mortality of HIV-infected patients starting potent antiretroviral therapy: comparison with the general population in nine industrialized countries.Int J Epidemiol. 2009 Dec;38(6):1624-33. doi: 10.1093/ije/dyp306. Epub 2009 Oct 9. Int J Epidemiol. 2009. PMID: 19820106 Free PMC article.
-
The effect of injecting drug use history on disease progression and death among HIV-positive individuals initiating combination antiretroviral therapy: collaborative cohort analysis.HIV Med. 2012 Feb;13(2):89-97. doi: 10.1111/j.1468-1293.2011.00940.x. Epub 2011 Aug 7. HIV Med. 2012. PMID: 21819529 Free PMC article.
-
Survival analysis of PLWHA undergoing combined antiretroviral therapy: exploring long-term prognosis and influencing factors.Front Public Health. 2024 Feb 22;12:1327264. doi: 10.3389/fpubh.2024.1327264. eCollection 2024. Front Public Health. 2024. PMID: 38454987 Free PMC article.
-
CD4 immunophenotyping in HIV infection.Nat Rev Microbiol. 2008 Nov;6(11 Suppl):S7-15. doi: 10.1038/nrmicro1998. Nat Rev Microbiol. 2008. PMID: 18923413 Free PMC article. Review.
-
Causes of death and risk factors for mortality among HIV-infected patients receiving antiretroviral therapy in Korea.J Korean Med Sci. 2013 Jul;28(7):990-7. doi: 10.3346/jkms.2013.28.7.990. Epub 2013 Jul 3. J Korean Med Sci. 2013. PMID: 23853480 Free PMC article.
References
-
- Hammer SM, Squires KE, Hughes MD, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. N Engl J Med. 1997;337:725–733. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet. 2003;362:22–29. - PubMed
-
- Sterne JA, Hernan MA, Ledergerber B, et al. Long-term effectiveness of potent antiretroviral therapy in preventing AIDS and death: a prospective cohort study. Lancet. 2005;366:378–384. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
