

Pharmacological treatment of chronic obstructive pulmonary disease
- PMID: 18044097
- PMCID: PMC2707800
- DOI: 10.2147/copd.2006.1.4.409
Pharmacological treatment of chronic obstructive pulmonary disease
Abstract
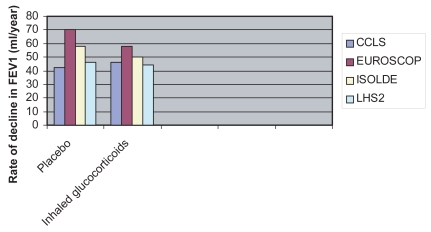
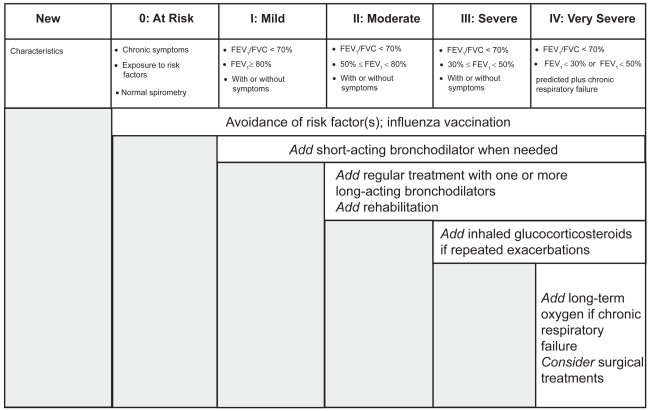
None of the drugs currently available for chronic obstructive pulmonary disease (COPD) are able to reduce the progressive decline in lung function which is the hallmark of this disease. Smoking cessation is the only intervention that has proved effective. The current pharmacological treatment of COPD is symptomatic and is mainly based on bronchodilators, such as selective beta2-adrenergic agonists (short- and long-acting), anticholinergics, theophylline, or a combination of these drugs. Glucocorticoids are not generally recommended for patients with stable mild to moderate COPD due to their lack of efficacy, side effects, and high costs. However, glucocorticoids are recommended for severe COPD and frequent exacerbations of COPD. New pharmacological strategies for COPD need to be developed because the current treatment is inadequate.
Figures

References
-
- Aaron SD, Vandemheen K, Fergusson D, et al. The Canadian Optimal Therapy for COPD trial: design, organization and patient recruitment. Can Respir J. 2004;11:581–5. - PubMed
-
- [ATS] American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995;152:S77–121. - PubMed
-
- Anthonisen NR, Connett JE, Kiley JP, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA. 1994;272:1497–505. - PubMed
-
- Anthonisen NR, Manfreda J, Warren CP, et al. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196–204. - PubMed
-
- Barbera JA, Reyes A, Roca J, et al. Effect of intravenously administered aminophylline on ventilation/perfusion inequality during recovery from exacerbations of chronic obstructive pulmonary disease. Am Rev Respir Dis. 1992;145:1328–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
