

Hemoglobin level variability: associations with mortality
- PMID: 18045862
- PMCID: PMC2390986
- DOI: 10.2215/CJN.01610407
Hemoglobin level variability: associations with mortality
Abstract
Background/objectives: Awareness of hemoglobin level variability in dialysis patients is increasing, as is interest in its potential implications. In this retrospective, national study of associations between the degree of hemoglobin level variability in the first 6 mo of 2004 and subsequent mortality rates in the following 6 mo, 159,720 hemodialysis patients receiving epoetin therapy were studied.
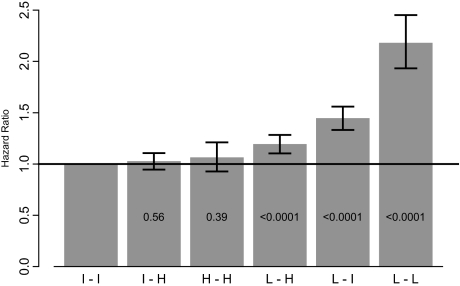
Design, setting, participants, measurements: Monthly hemoglobin values were categorized as low (L; < 11 g/dl), intermediate (I; 11 to 12.5 g/dl), and high (H; >12.5 g/dl). Variability groups were classified on the basis of the lowest and highest hemoglobin categories seen during the 6-mo observation period: low-low (L-L), 1.4%; intermediate-intermediate (I-I), 6.0%; high-high (H-H), 2.3%; low-intermediate (L-I), 18.3%; intermediate-high (I-H), 31.7%, and low-high (L-H), 40.2%.
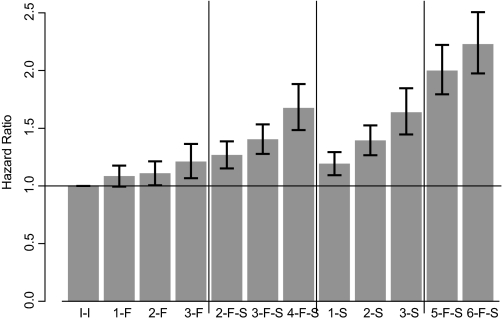
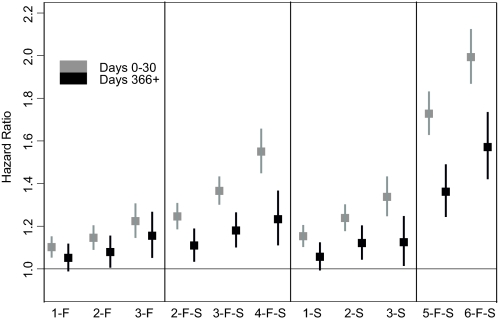
Results: On multivariate analysis, adjusted hazards ratios for subsequent mortality events were as follows: I-I, 1.0 (reference category); I-H, 1.02 (95% confidence interval [CI] 0.95 to 1.11); H-H, 1.06 (95% CI 0.93 to 1.21); L-H, 1.19 (95% CI 1.10 to 1.28); L-I, 1.44 (95% CI 1.33 to 1.56), and L-L, 2.18 (95% CI 1.93 to 2.45). Persistently and transiently low hemoglobin levels and highly variable hemoglobin levels were associated with increased risk of death; transiently and persistently high hemoglobin levels were not associated with increased risk of death. Bayesian modeling indicated that > or =3 mo with hemoglobin levels <11 g/dl may be associated with of increased risk of death.
Conclusions: Number of months with hemoglobin values below the target range, rather than hemoglobin variability itself, may be the primary driver of increased risk of death. Further research is needed to distinguish cause from effect and to understand the underlying mechanisms.
Figures
Comment in
-
Anemia of chronic kidney disease.Clin J Am Soc Nephrol. 2008 Jan;3(1):3-6. doi: 10.2215/CJN.05131107. Epub 2007 Dec 12. Clin J Am Soc Nephrol. 2008. PMID: 18077779 No abstract available.
References
-
- Collins AJ, Li S, Ebben J, Ma JX, Manning W: Hematocrit levels and associated Medicare expenditures. Am J Kidney Dis 36: 282–293, 2000 - PubMed
-
- Ma JZ, Ebben J, Xia H, Collins AJ: Hematocrit level and associated mortality in hemodialysis patients. J Am Soc Nephrol 10: 610–619, 1999 - PubMed
-
- Madore F, Lowrie EG, Brugnara C, Lew NL, Lazarus JM, Bridges K, Owen WF: Anemia in hemodialysis patients: Variables affecting this outcome predictor. J Am Soc Nephrol 8: 1921–1929, 1997 - PubMed
-
- Ofsthun N, Labrecque J, Lacson E, Keen M, Lazarus JM: The effects of higher hemoglobin levels on mortality and hospitalization in hemodialysis patients. Kidney Int 63: 1908–1914, 2003 - PubMed
-
- Regidor DL, Kopple JD, Kovesdy CP, Kilpatrick RD, McAllister CJ, Aronovitz J, Greenland S, Kalantar-Zadeh K: Associations between changes in hemoglobin and administered erythropoiesis-stimulating agent and survival in hemodialysis patients. J Am Soc Nephrol 17: 1181–1191, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
