

Testing NMDA receptor block as a therapeutic strategy for reducing ischaemic damage to CNS white matter
- PMID: 18046734
- PMCID: PMC2863073
- DOI: 10.1002/glia.20608
Testing NMDA receptor block as a therapeutic strategy for reducing ischaemic damage to CNS white matter
Abstract
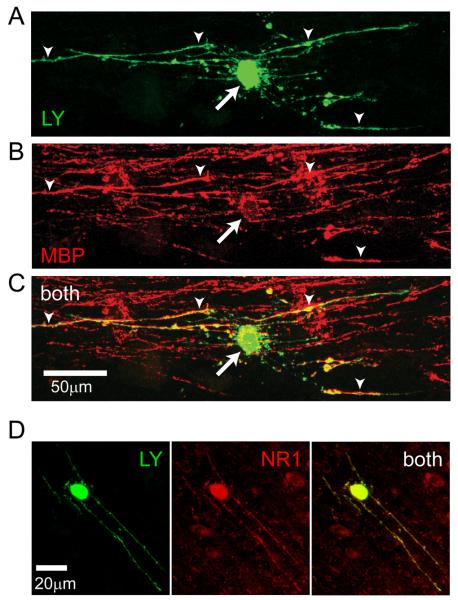
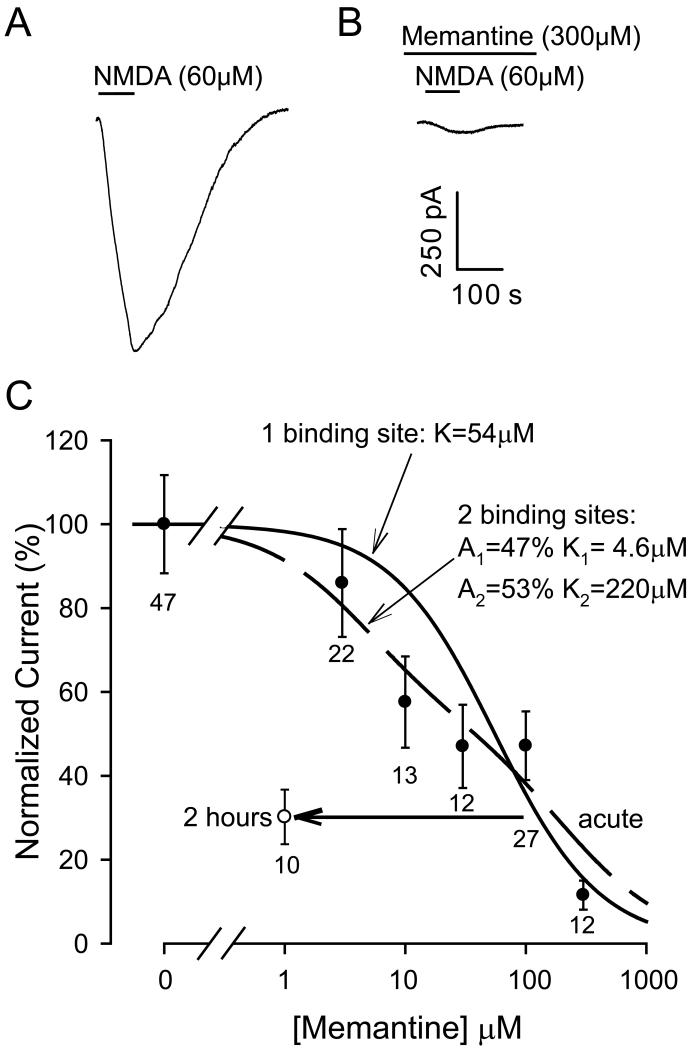
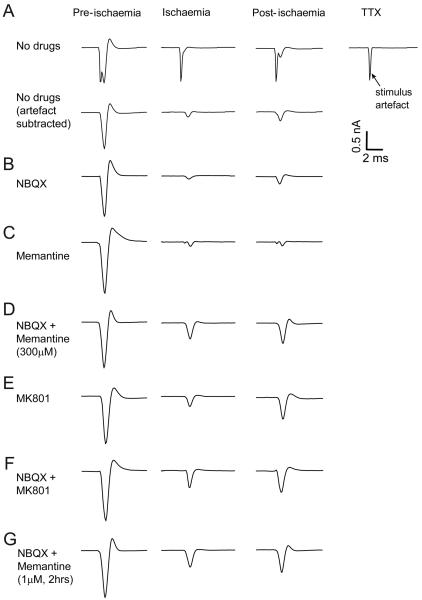
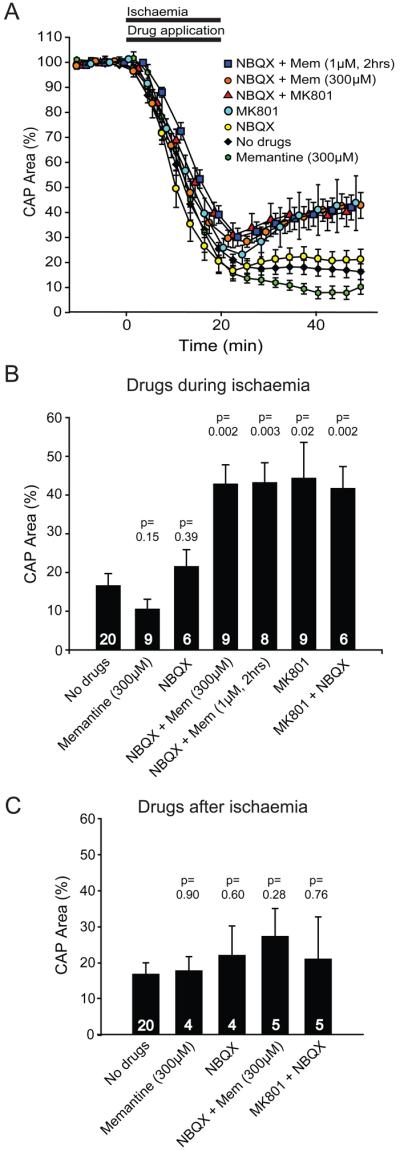
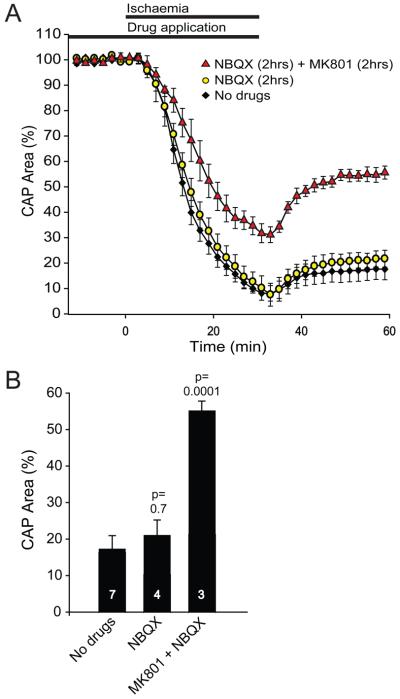
Damage to oligodendrocytes caused by glutamate release contributes to mental or physical handicap in periventricular leukomalacia, spinal cord injury, multiple sclerosis, and stroke, and has been attributed to activation of AMPA/kainate receptors. However, glutamate also activates unusual NMDA receptors in oligodendrocytes, which can generate an ion influx even at the resting potential in a physiological [Mg2+]. Here, we show that the clinically licensed NMDA receptor antagonist memantine blocks oligodendrocyte NMDA receptors at concentrations achieved therapeutically. Simulated ischaemia released glutamate which activated NMDA receptors, as well as AMPA/kainate receptors, on mature and precursor oligodendrocytes. Although blocking AMPA/kainate receptors alone during ischaemia had no effect, combining memantine with an AMPA/kainate receptor blocker, or applying the NMDA blocker MK-801 alone, improved recovery of the action potential in myelinated axons after the ischaemia. These data suggest NMDA receptor blockers as a potentially useful treatment for some white matter diseases and define conditions under which these blockers may be useful therapeutically. Our results highlight the importance of developing new antagonists selective for oligodendrocyte NMDA receptors based on their difference in subunit structure from most neuronal NMDA receptors.
Copyright (c) 2007 Wiley-Liss, Inc.
Figures

References
-
- Back SA, Craig A, Kayton RJ, Luo NL, Meshul CK, Allcock N, Fern R. Hypoxia-ischemia preferentially triggers glutamate depletion from oligodendroglia and axons in perinatal cerebral white matter. J Cereb Blood Flow Metab. 2007;27:334–347. - PubMed
-
- Blanpied TA, Boeckman FA, Aizenman E, Johnson JW. Trapping block of NMDA-activated responses by amantadine and memantine. J Neurophysiol. 1997;77:309–323. - PubMed
-
- Bolton S, Butt AM. The optic nerve: a model for axon-glia interactions. J Pharm Toxicol Meth. 2005;51:221–233. - PubMed
-
- Craig A, Ling Luo N, Beardsley DJ, Wingate-Pearse N, Walker DW, Hohimer AR, Back SA. Quantitative analysis of perinatal rodent oligodendrocyte lineage progression and its correlation with human. Exp Neurol. 2003;181:231–240. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
