

Tiotropium bromide
- PMID: 18046887
- PMCID: PMC2706608
- DOI: 10.2147/copd.2006.1.2.107
Tiotropium bromide
Abstract
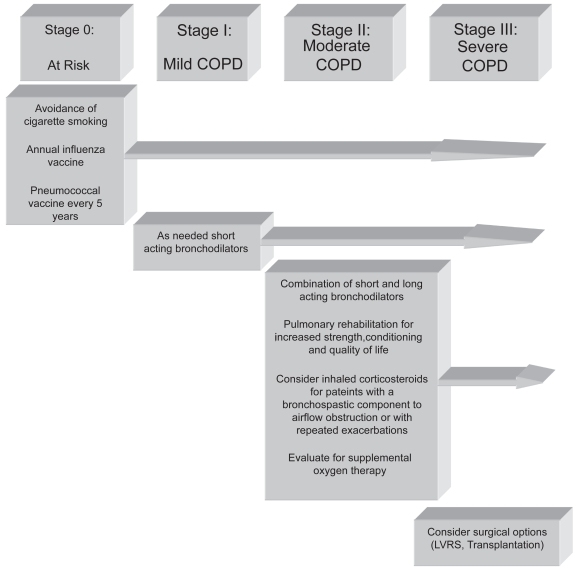
Therapy with bronchodilators forms the pharmacologic foundation of the treatment of patients with COPD. Bronchodilators can significantly lessen dyspnea, increase airflow, improve quality of life, and enhance exercise performance. While bronchodilators decrease airway resistance and lessen dynamic hyperinflation in patients with COPD, they have not been shown to alter the rate of decline in FEV1 over time, or improve patient survival. Fairly recently, a long-acting, once-daily anticholinergic medication, tiotropium bromide, has been developed which may improve symptom management in COPD patients. This paper reviews anticholinergic pharmacologic therapy for patients with COPD focusing on tiotropium bromide, and discusses treatment strategies based on disease stage. It is important to recognize that while bronchodilators improve symptoms, a multimodality treatment approach including respiratory and rehabilitative therapy, nutrition services, psychosocial counseling, and surgical care, is often necessary for the best possible care of patients with COPD.
Figures
Similar articles
-
The role of tiotropium bromide, a long-acting anticholinergic bronchodilator, in the management of COPD.Treat Respir Med. 2005;4(4):275-81. doi: 10.2165/00151829-200504040-00005. Treat Respir Med. 2005. PMID: 16086600 Review.
-
Tiotropium bromide. A review of its use as maintenance therapy in patients with COPD.Treat Respir Med. 2004;3(4):247-68. doi: 10.2165/00151829-200403040-00005. Treat Respir Med. 2004. PMID: 15350163 Review.
-
Redefining treatment in COPD: new directions in bronchodilator therapy.Treat Respir Med. 2004;3(2):89-95. doi: 10.2165/00151829-200403020-00003. Treat Respir Med. 2004. PMID: 15182210 Review.
-
[Clinical benefits of tiotropium, a new anticholinergic bronchodilator].An Med Interna. 2002 Dec;19(12):640-3. An Med Interna. 2002. PMID: 12593035 Review. Spanish.
-
[Pharmacological and clinical profile of tiotropium bromide (Spiriva), a new long-acting anticholinergic bronchodilator for COPD treatment].Nihon Yakurigaku Zasshi. 2005 May;125(5):307-13. doi: 10.1254/fpj.125.307. Nihon Yakurigaku Zasshi. 2005. PMID: 15997169 Japanese. No abstract available.
Cited by
-
Pharmacotherapies for COPD.Clin Med Insights Circ Respir Pulm Med. 2013 Apr 25;7:17-34. doi: 10.4137/CCRPM.S7211. Print 2013. Clin Med Insights Circ Respir Pulm Med. 2013. PMID: 23700381 Free PMC article.
-
Assessment of bronchodilator responsiveness to salbutamol or ipratropium using different criteria in treatment-naïve patients with asthma and COPD.Eur Clin Respir J. 2024 Mar 21;11(1):2328434. doi: 10.1080/20018525.2024.2328434. eCollection 2024. Eur Clin Respir J. 2024. PMID: 38529514 Free PMC article.
References
-
- ACCP/AACVPR Pulmonary Rehabilitation Guidelines Panel. Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based guidelines. Chest. 1997;112:1363–96. - PubMed
-
- [ATS] American Thoracic Society. Statement: Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Care Med. 1995;152(Suppl):77–121. - PubMed
-
- [ATS] American Thoracic Society. Official Statement: Pulmonary rehabilitation-1999. Am J Respir Crit Care Med. 1999;159:1666–82. - PubMed
-
- Anthonisen NR, Connett JE, Kiley JP, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA. 1994;272:1497–505. - PubMed
-
- Anthonisen NR, Connett JE, Enright PL, et al. Lung Health Study Research Group. Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med. 2002;166:333–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
