

Eosinophilic airway inflammation in COPD
- PMID: 18046901
- PMCID: PMC2706606
- DOI: 10.2147/copd.2006.1.1.39
Eosinophilic airway inflammation in COPD
Abstract
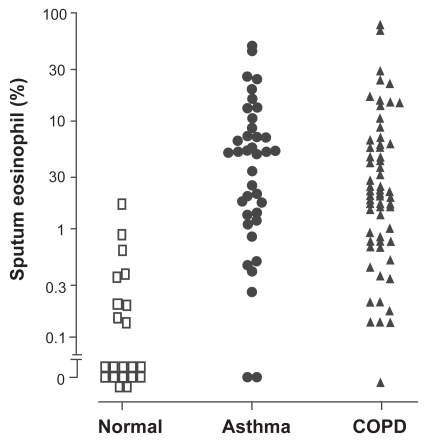
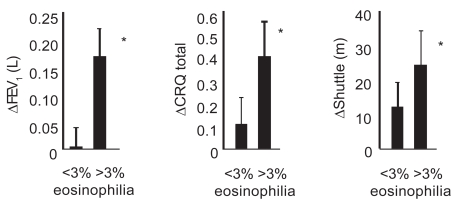
Chronic obstructive pulmonary disease is a common condition and a major cause of mortality. COPD is characterized by irreversible airflow obstruction. The physiological abnormalities observed in COPD are due to a combination of emphysema and obliteration of the small airways in association with airway inflammation. The predominant cells involved in this inflammatory response are CD8+ lymphocytes, neutrophils, and macrophages. Although eosinophilic airway inflammation is usually considered a feature of asthma, it has been demonstrated in large and small airway tissue samples and in 20%-40% of induced sputum samples from patients with stable COPD. This airway eosinophilia is increased in exacerbations. Thus, modifying eosinophilic inflammation may be a potential therapeutic target in COPD. Eosinophilic airway inflammation is resistant to inhaled corticosteroid therapy, but does respond to systemic corticosteroid therapy, and the degree of response is related to the intensity of the eosinophilic inflammation. In COPD, targeting treatment to normalize the sputum eosinophilia reduced the number of hospital admissions. Whether controlling eosinophilic inflammation in COPD patients with an airway eosinophilia will modify disease progression and possibly alter mortality is unknown, but warrants further investigation.
Figures
References
-
- Balbi B, Majori M, Bertacco S, et al. Inhaled corticosteroids in stable COPD patients: do they have effects on cells and molecular mediators of airway inflammation? Chest. 2000;117:1633–7. - PubMed
-
- Balzano G, Stefanelli F, Iorio C, et al. Eosinophilic inflammation in stable chronic obstructive pulmonary disease. Relationship with neutrophils and airway function. Am J Respir Crit Care Med. 1999;160(5Pt1):1486–92. - PubMed
-
- Barnes NC. Inhaled steroids in COPD. Lancet. 1998;351:766–7. - PubMed
-
- Barnes NC, Qui Y, Pavord I, et al. Salmeterol/fluticasone proprionate: anti-inflammatory effects in COPD. Proc Am Thorac Soc. 2005;2:A543.
-
- Barnes PJ, Ito K, Adcock IM. Corticosteroid resistance in chronic obstructive pulmonary disease: inactivation of histone deacetylase. Lancet. 2004;363:731–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
