

When do HIV-infected women disclose their HIV status to their male partner and why? A study in a PMTCT programme, Abidjan
- PMID: 18052603
- PMCID: PMC2100145
- DOI: 10.1371/journal.pmed.0040342
When do HIV-infected women disclose their HIV status to their male partner and why? A study in a PMTCT programme, Abidjan
Abstract
Background: In Africa, women tested for HIV during antenatal care are counselled to share with their partner their HIV test result and to encourage partners to undertake HIV testing. We investigate, among women tested for HIV within a prevention of mother-to-child transmission of HIV (PMTCT) programme, the key moments for disclosure of their own HIV status to their partner and the impact on partner HIV testing.
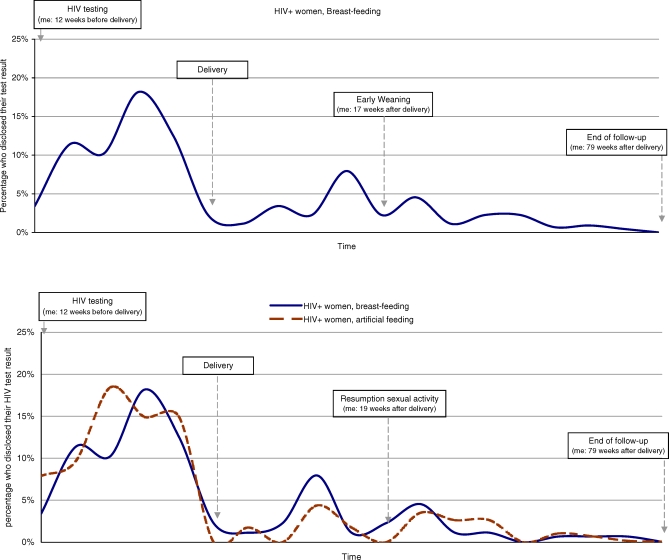
Methods and findings: Within the Ditrame Plus PMTCT project in Abidjan, 546 HIV-positive and 393 HIV-negative women were tested during pregnancy and followed-up for two years after delivery. Circumstances, frequency, and determinants of disclosure to the male partner were estimated according to HIV status. The determinants of partner HIV testing were identified according to women's HIV status. During the two-year follow-up, disclosure to the partner was reported by 96.7% of the HIV-negative women, compared to 46.2% of HIV-positive women (chi(2) = 265.2, degrees of freedom [df] = 1, p < 0.001). Among HIV-infected women, privileged circumstances for disclosure were just before delivery, during early weaning (at 4 mo to prevent HIV postnatal transmission), or upon resumption of sexual activity. Formula feeding by HIV-infected women increased the probability of disclosure (adjusted odds ratio 1.54, 95% confidence interval 1.04-2.27, Wald test = 4.649, df = 1, p = 0.031), whereas household factors such as having a co-spouse or living with family reduced the probability of disclosure. The proportion of male partners tested for HIV was 23.1% among HIV-positive women and 14.8% among HIV-negative women (chi(2) = 10.04, df = 1, p = 0.002). Partners of HIV-positive women who were informed of their wife's HIV status were more likely to undertake HIV testing than those not informed (37.7% versus 10.5%, chi(2) = 56.36, df = 1, p < 0.001).
Conclusions: In PMTCT programmes, specific psychosocial counselling and support should be provided to women during the key moments of disclosure of HIV status to their partners (end of pregnancy, weaning, and resumption of sexual activity). This support could contribute to improving women's adherence to the advice given to prevent postnatal and sexual HIV transmission.
Conflict of interest statement
Figures
Comment in
-
HIV treatment proceeds as prevention research confounds.PLoS Med. 2007 Dec;4(12):e347. doi: 10.1371/journal.pmed.0040347. PLoS Med. 2007. PMID: 18052606 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO). AIDS epidemic update: December 2006. Geneva: UNAIDS/WHO; 2006. Available: http://data.unaids.org/pub/EpiReport/2006/2006_EpiUpdate_en.pdf. Accessed 7 December 2006.
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) Intensifying HIV prevention: a UNAIDS policy position paper. Geneva: UNAIDS; 2005. Available: http://www.unaids.org/en/publications/default.asp. Accessed 7 December 2006.
-
- Tabi MM, Frimpong S. HIV infection of women in Africa countries. Int Nurs Rev. 2003;50:242–250. - PubMed
-
- Bauni EK, Obonyo BJ. The low acceptability and use of condom within marriage: evidence from Nakuru District, Kenya. Etude Popul Afr. 2003;18:51–65.
-
- Muhwava W. Condom use within marriage and consensual unions in the era of HIV/AIDS in Zimbabwe. Etude Popul Afr. 2004;19:118–141.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
