

Assessment of recent HIV-1 infection by a line immunoassay for HIV-1/2 confirmation
- PMID: 18052604
- PMCID: PMC2100138
- DOI: 10.1371/journal.pmed.0040343
Assessment of recent HIV-1 infection by a line immunoassay for HIV-1/2 confirmation
Abstract
Background: Knowledge of the number of recent HIV infections is important for epidemiologic surveillance. Over the past decade approaches have been developed to estimate this number by testing HIV-seropositive specimens with assays that discriminate the lower concentration and avidity of HIV antibodies in early infection. We have investigated whether this "recency" information can also be gained from an HIV confirmatory assay.
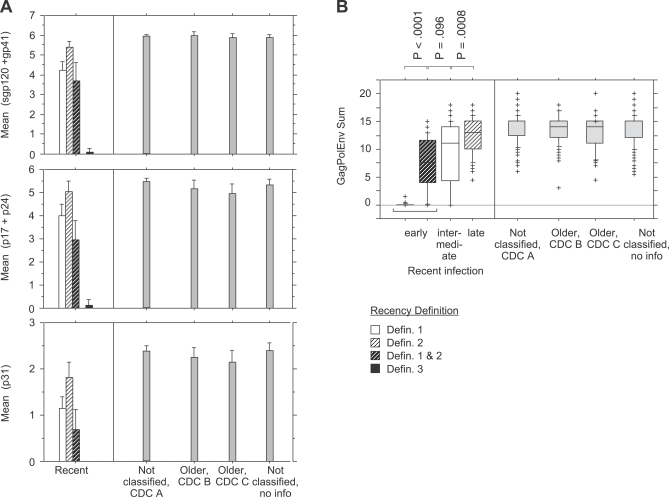
Methods and findings: The ability of a line immunoassay (INNO-LIA HIV I/II Score, Innogenetics) to distinguish recent from older HIV-1 infection was evaluated in comparison with the Calypte HIV-1 BED Incidence enzyme immunoassay (BED-EIA). Both tests were conducted prospectively in all HIV infections newly diagnosed in Switzerland from July 2005 to June 2006. Clinical and laboratory information indicative of recent or older infection was obtained from physicians at the time of HIV diagnosis and used as the reference standard. BED-EIA and various recency algorithms utilizing the antibody reaction to INNO-LIA's five HIV-1 antigen bands were evaluated by logistic regression analysis. A total of 765 HIV-1 infections, 748 (97.8%) with complete test results, were newly diagnosed during the study. A negative or indeterminate HIV antibody assay at diagnosis, symptoms of primary HIV infection, or a negative HIV test during the past 12 mo classified 195 infections (26.1%) as recent (< or = 12 mo). Symptoms of CDC stages B or C classified 161 infections as older (21.5%), and 392 patients with no symptoms remained unclassified. BED-EIA ruled 65% of the 195 recent infections as recent and 80% of the 161 older infections as older. Two INNO-LIA algorithms showed 50% and 40% sensitivity combined with 95% and 99% specificity, respectively. Estimation of recent infection in the entire study population, based on actual results of the three tests and adjusted for a test's sensitivity and specificity, yielded 37% for BED-EIA compared to 35% and 33% for the two INNO-LIA algorithms. Window-based estimation with BED-EIA yielded 41% (95% confidence interval 36%-46%).
Conclusions: Recency information can be extracted from INNO-LIA-based confirmatory testing at no additional costs. This method should improve epidemiologic surveillance in countries that routinely use INNO-LIA for HIV confirmation.
Conflict of interest statement
Figures
Comment in
-
HIV treatment proceeds as prevention research confounds.PLoS Med. 2007 Dec;4(12):e347. doi: 10.1371/journal.pmed.0040347. PLoS Med. 2007. PMID: 18052606 Free PMC article.
References
-
- Janssen RS, Satten GA, Stramer SL, Rawal BD, O'Brien TR, et al. New testing strategy to detect early HIV-1 infection for use in incidence estimates and for clinical and prevention purposes. JAMA. 1998;280:42–48. - PubMed
-
- Parekh BS, McDougal JS. Application of laboratory methods for estimation of HIV-1 incidence. Indian J Med Res. 2005;121:510–518. - PubMed
-
- Parekh BS, Kennedy MS, Dobbs T, Pau CP, Byers R, et al. Quantitative detection of increasing HIV type 1 antibodies after seroconversion: a simple assay for detecting recent HIV infection and estimating incidence. AIDS Res Hum Retroviruses. 2002;18:295–307. - PubMed
-
- Schupbach J, Popovic M, Gilden RV, Gonda MA, Sarngadharan MG, et al. Serological analysis of a subgroup of human T-lymphotropic retroviruses (HTLV-III) associated with AIDS. Science. 1984;224:503–505. - PubMed
-
- Sarngadharan MG, Popovic M, Bruch L, Schupbach J, Gallo RC. Antibodies reactive with human T-lymphotropic retroviruses (HTLV-III) in the serum of patients with AIDS. Science. 1984;224:506–508. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
