

Two sisters with idiopathic pulmonary hemosiderosis
- PMID: 18060095
- PMCID: PMC2677775
- DOI: 10.1155/2007/150926
Two sisters with idiopathic pulmonary hemosiderosis
Abstract
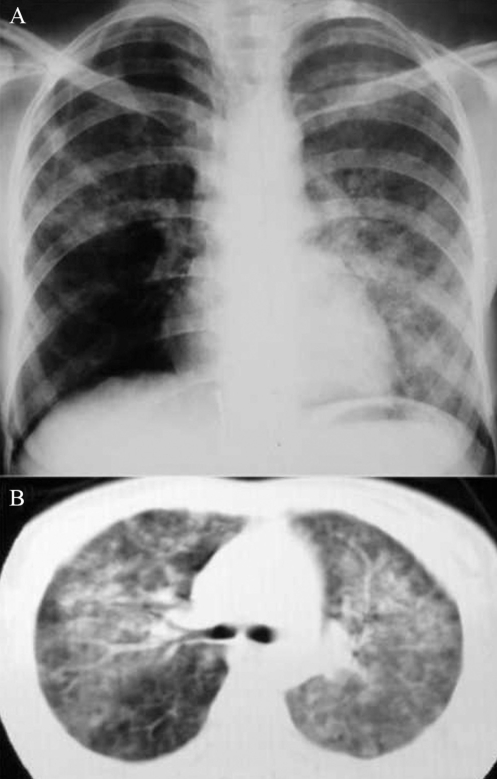
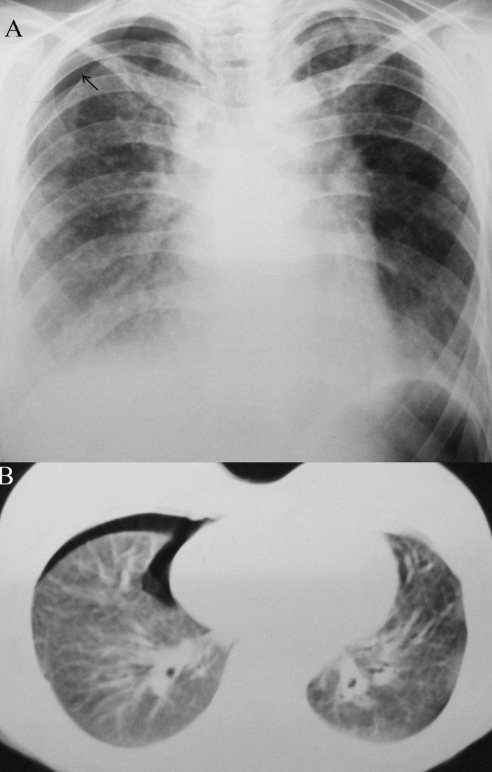
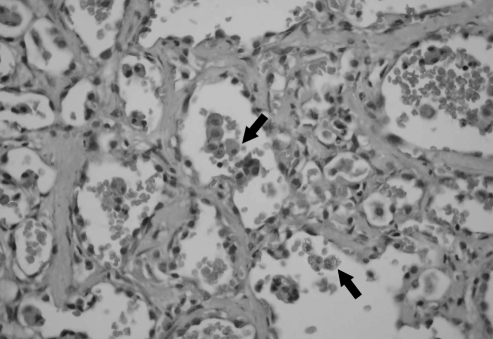
Idiopathic pulmonary hemosiderosis (IPH) is a rare cause of diffuse alveolar hemorrhage with unknown etiology. In the present report, the presentations of two sisters are described: one sister had IPH, eosinophilia and a high serum immunoglobulin E (IgE) level; and the other had IPH, pneumothorax, eosinophilia and a high serum IgE level. Both cases had quite unusual presentations. The first patient was 23 years of age, and had suffered from dry cough and progressive dyspnea for four years. Her hemoglobin level was 60 g/L, total serum IgE level was 900 U/mL and eosinophilia was 9%. Her chest radiography revealed diffuse infiltration. She died due to respiratory failure. The second patient was 18 years of age. She had also suffered from dry cough and gradually increasing dyspnea for two years. She had partial pneumothorax in the right lung and diffuse infiltration in other pulmonary fields on chest radiography. Her hemoglobin level was 99 g/L, total serum IgE level was 1200 U/mL and eosinophilia was 8%. IPH was diagnosed by open lung biopsy. All these findings suggested that familial or allergic factors, as well as immunological factors, might have contributed to the etiology of IPH.
L’hémosidérose pulmonaire idiopathique (HPI) est une cause rare d’hémorragie alvéolaire diffuse à l’étiologie inconnue. Dans le présent article, les auteurs décrivent la présentation de deux sœurs : l’une souffrait d’HPI, d’éosinophilie et d’un taux élevé d’immunoglobuline E (IgE) sérique et l’autre, d’HPI, d’un pneumothorax, d’une éosinophilie et d’un taux élevé d’IgE sérique. Les deux cas avaient une présentation très inhabituelle. La première patiente avait 23 ans et était incommodée par une toux sèche et une dyspnée évolutive depuis quatre ans. Son taux d’hémoglobine était de 60 g/L, son taux d’IgE sérique total, de 900 U/mL, et son éosinophilie, de 9 %. La radiographie pulmonaire révélait une infiltration diffuse. Elle est morte d’une insuffisance respiratoire. La deuxième patiente avait 18 ans. Elle souffrait également d’une toux sèche et d’une dyspnée croissante depuis deux ans. Elle avait un pneumothorax partiel dans un poumon et une infiltration diffuse dans les autres champs pulmonaires selon la radiographie pulmonaire. Son taux d’hémoglobine était de 99 g/L, son taux d’IgE sérique total, de 1 200 U/mL, et son éosinophilie, de 8 %. L’HPI a été diagnostiquée par une biopsie pulmonaire ouverte. Toutes ces observations indiquent que des facteurs familiaux ou allergiques, en plus des facteurs immunologiques, pourraient avoir contribué à l’étiologie de l’HPI.
Figures
References
-
- Ferrari GF, Fioretto JR, Alves AF, Brandão GS. [Idiopathic pulmonary hemosiderosis: Case report.] J Pediatr (Rio J) 2000;76:149–52. - PubMed
-
- Cohen S. Idiopathic pulmonary hemosiderosis. Am J Med Sci. 1999;317:67–74. - PubMed
-
- Ioachimescu OC, Sieber S, Kotch A. Idiopathic pulmonary haemosiderosis revisited. Eur Respir J. 2004;24:162–70. - PubMed
-
- Vinodh BN, Sharma SK, Mukhopadhyay S, Ray R. Idiopathic pulmonary haemosiderosis: Two case reports. Indian J Chest Dis Allied Sci. 2006;48:75–7. - PubMed
-
- Dearborn DG. Pulmonary hemosiderosis. In: Behrman RE, Kliegman RM, Jenson HB, editors. Nelson Textbook of Pediatrics. Philadelphia: WB Saunders Co; 2003. pp. 1455–7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
