

Esophageal dysmotility in patients who have eosinophilic esophagitis
- PMID: 18061103
- PMCID: PMC3001401
- DOI: 10.1016/j.giec.2007.09.006
Esophageal dysmotility in patients who have eosinophilic esophagitis
Abstract
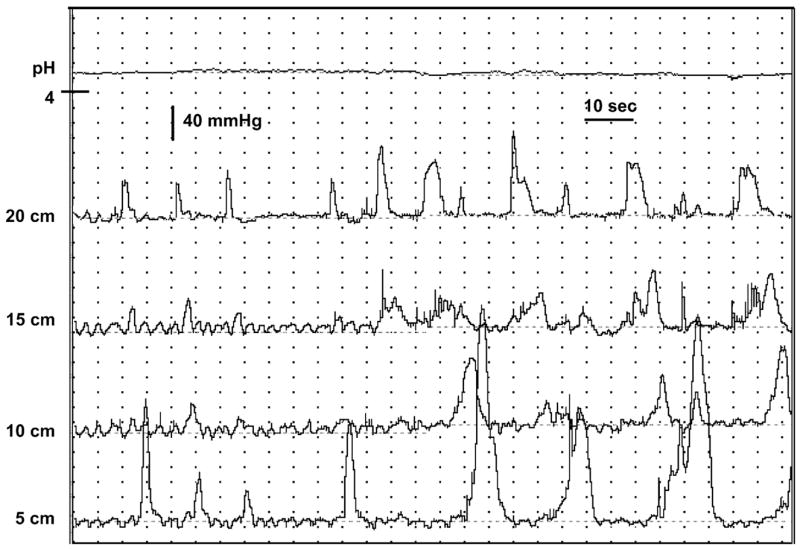
The understanding of esophageal motility alterations in patients who have eosinophilic esophagitis (EE) is in its infancy despite the common presenting complaint of dysphagia. A diversity of motility disorders has been reported in patients who have EE including achalasia, diffuse esophageal spasm, nutcracker esophagus, and nonspecific motility alterations including high-amplitude esophageal body contractions, tertiary contractions, abnormalities in lower esophageal sphincter pressure, and other peristaltic problems. Some evidence suggests that treatment of EE will improve motility. Technological advances such as high-resolution manometry and combined manometry with impedance may provide new insight into more subtle motility abnormalities.
Figures
Similar articles
-
Prevalence of esophageal dysmotility in a cohort of patients with esophageal biopsies consistent with eosinophilic esophagitis.Dis Esophagus. 2009;22(6):543-8. doi: 10.1111/j.1442-2050.2009.00949.x. Epub 2009 Mar 6. Dis Esophagus. 2009. PMID: 19302212
-
Esophageal motility in eosinophilic esophagitis.Rev Gastroenterol Mex. 2015 Jul-Sep;80(3):205-13. doi: 10.1016/j.rgmx.2015.05.005. Epub 2015 Aug 12. Rev Gastroenterol Mex. 2015. PMID: 26275635 Review. English, Spanish.
-
Manometric findings in adult eosinophilic oesophagitis: a study of 12 cases.Eur J Gastroenterol Hepatol. 2007 May;19(5):417-24. doi: 10.1097/MEG.0b013e328010bd69. Eur J Gastroenterol Hepatol. 2007. PMID: 17413294
-
Muscle layer histopathology and manometry pattern of primary esophageal motility disorders including achalasia.Neurogastroenterol Motil. 2017 Mar;29(3). doi: 10.1111/nmo.12968. Epub 2016 Oct 3. Neurogastroenterol Motil. 2017. PMID: 27699951
-
Esophageal Motility Disorders.Am Fam Physician. 2020 Sep 1;102(5):291-296. Am Fam Physician. 2020. PMID: 32866357 Review.
Cited by
-
Manometric features of eosinophilic esophagitis in esophageal pressure topography.Neurogastroenterol Motil. 2011 Mar;23(3):208-14, e111. doi: 10.1111/j.1365-2982.2010.01633.x. Epub 2010 Nov 23. Neurogastroenterol Motil. 2011. PMID: 21091849 Free PMC article.
-
Esophageal polyp in a teenage boy with eosinophilic esophagitis.SAGE Open Med Case Rep. 2022 Aug 12;10:2050313X221116954. doi: 10.1177/2050313X221116954. eCollection 2022. SAGE Open Med Case Rep. 2022. PMID: 35991956 Free PMC article.
-
Eosinophilic esophagitis.World J Gastroenterol. 2009 Jan 7;15(1):17-24. doi: 10.3748/wjg.15.17. World J Gastroenterol. 2009. PMID: 19115464 Free PMC article. Review.
-
Esophageal dysmotility in patients with eosinophilic esophagitis: pathogenesis, assessment tools, manometric characteristics, and clinical implications.Esophagus. 2023 Jan;20(1):29-38. doi: 10.1007/s10388-022-00964-z. Epub 2022 Oct 11. Esophagus. 2023. PMID: 36220921 Free PMC article. Review.
-
Association of achalasia and eosinophilic esophagitis.Indian J Gastroenterol. 2013 Jan;32(1):54-7. doi: 10.1007/s12664-012-0255-4. Epub 2012 Oct 3. Indian J Gastroenterol. 2013. PMID: 23054948
References
-
- Noel RJ, Putnam PE, Collins MH, Assa’ad AH, Guajardo JR, Jameson SC, et al. Clinical and immunopathologic effects of swallowed fluticasone for eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2004;2(7):568–75. - PubMed
-
- Khan S, Orenstein SR, Di Lorenzo C, Kocoshis S, Putnam PE, Sigurdsson L, et al. Eosinophilic Esophagitis. Strictures, Impactions, Dysphagia Dig Dis Sci. 2003;48:22–29. - PubMed
-
- Sgouros SN, Bergele C, Mantides A. Eosinophilic esophagitis in adults: a systematic review. Eur J Gastroenterol Hepatol. 2006;18(2):211–7. - PubMed
-
- Walsh SV, Antonioli DA, Goldman H, Fox VL, Bousvaros A, Leichtner AM, et al. Allergic esophagitis in children: a clinicopathological entity. Am J Surg Pathol. 1999;23(4):390–6. - PubMed
-
- Teitelbaum JE, Fox VL, Twarog FJ, Nurko S, Antonioli D, Gleich G, et al. Eosinophilic esophagitis in children: immunopathological analysis and response to fluticasone propionate. Gastroenterology. 2002;122(5):1216–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
