

Immunoregulatory factors in multiple sclerosis patients during and after pregnancy: relevance of natural killer cells
- PMID: 18062798
- PMCID: PMC2276950
- DOI: 10.1111/j.1365-2249.2007.03555.x
Immunoregulatory factors in multiple sclerosis patients during and after pregnancy: relevance of natural killer cells
Abstract
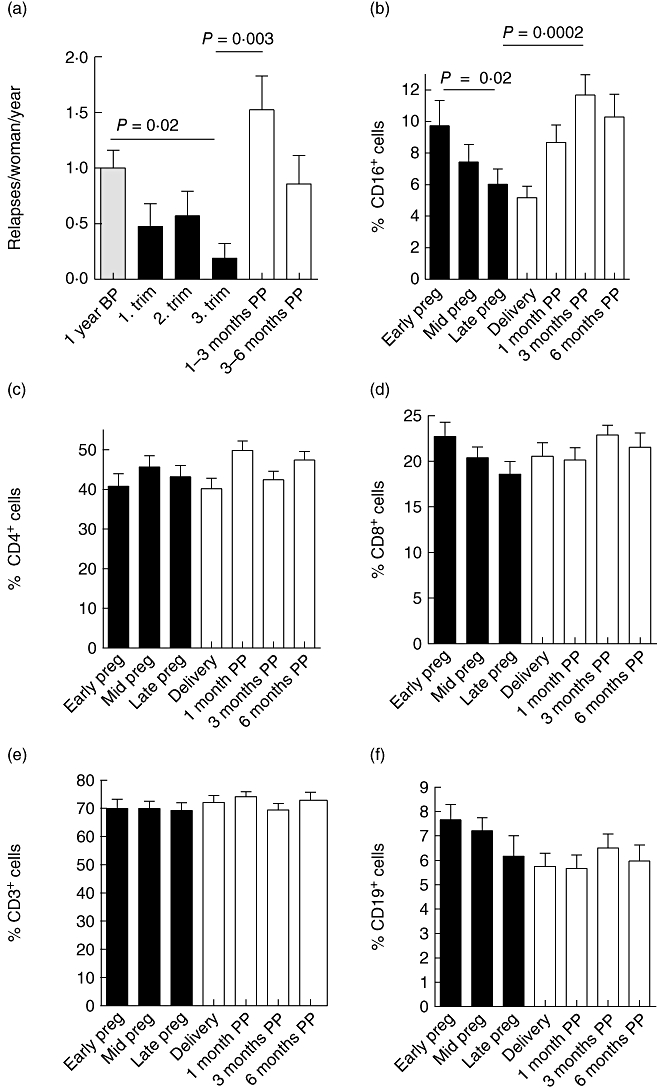
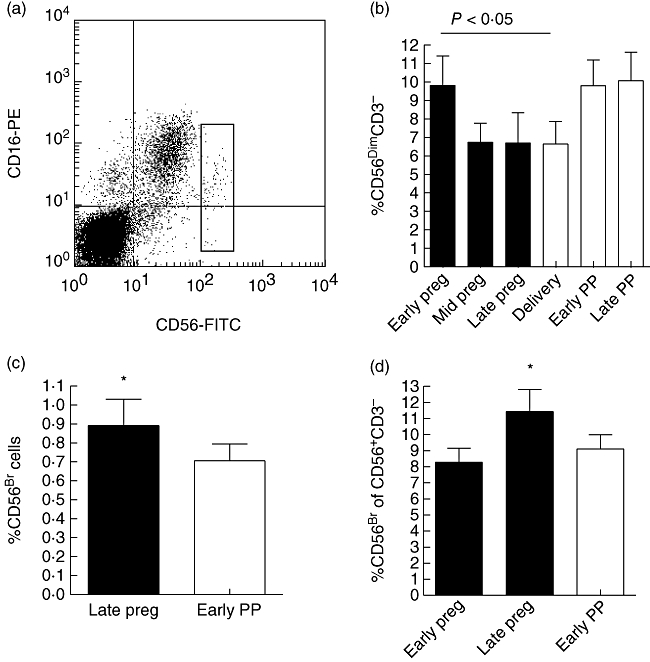
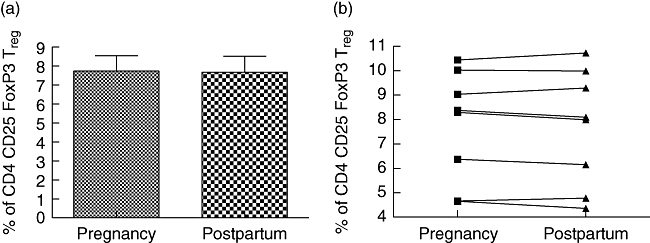
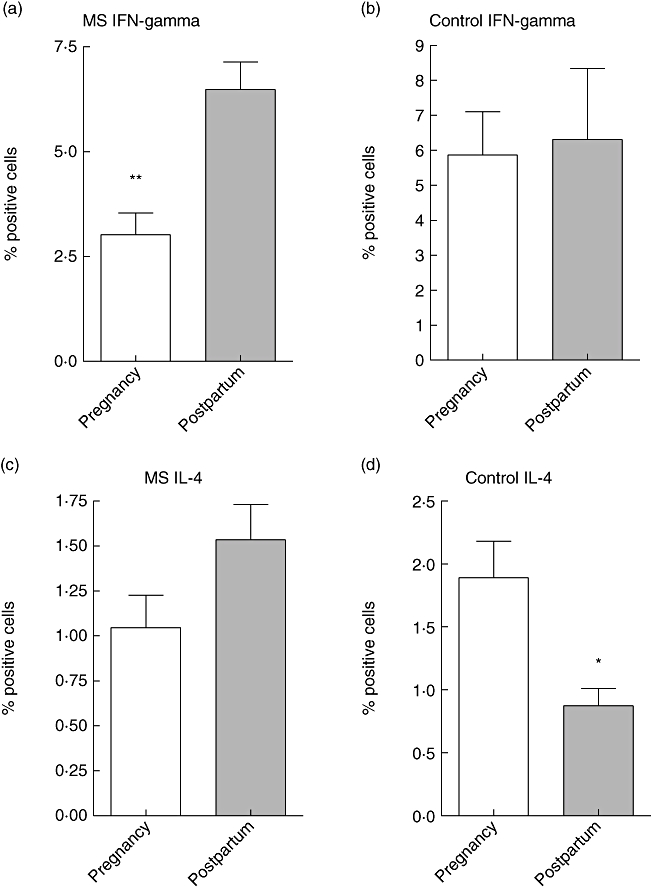
Multiple sclerosis (MS) ameliorates typically during pregnancy but after the delivery the relapse rate often increases. Our study was conducted to understand the immunoregulatory mechanisms accompanying this phenomenon. MS patients were followed-up prospectively during pregnancy and 6 months postpartum, with immunological characterization of the peripheral blood. Groups of age- and parity-matched healthy pregnant women, and age- and sex-matched non-pregnant women and non-pregnant MS patients were studied as controls. In our patient cohort, the annualized relapse rate was 1.0 +/- 1.0 relapses/woman/year (mean +/- standard deviation) during the year before pregnancy, but dropped to 0.2 +/- 0.9 during the third trimester (P = 0.02). After the delivery the relapse rate increased again to 1.4 +/- 1.9 (1-3 months postpartum versus third trimester P = 0.003). While percentages of peripheral blood CD3, CD4, CD8 and CD19 immune cell subsets were unchanged over the observation period, reduced disease activity during the last trimester was associated with a significant increase in the percentage of circulating CD56(bright) natural killer (NK) cells. Simultaneously, the proportion of circulating CD56(dim) NK cells was clearly reduced. No alteration was noted in CD4+ CD25(high) forkhead box P3+ regulatory T cells. Production of interferon-gamma by peripheral blood lymphocytes was down-regulated significantly during pregnancy in comparison to the postpartum period, resulting in an increased T helper type 2 (Th2) : Th1 ratio during pregnancy. In conclusion, pregnant state in MS patients is characterized by an increase in the percentage of CD56(bright) NK cells and by enhanced Th2 type cytokine secretion. Our findings suggest a potential role for CD56(bright) regulatory NK cells in the control of autoimmune inflammation during pregnancy in MS.
Figures
References
-
- Confavreux C, Hutchinson M, Hours MM, Cortinovis-Tourniaire P, Moreau T. Rate of pregnancy-related relapse in multiple sclerosis. N Engl J Med. 1998;339:285–91. Pregnancy Multiple Sclerosis Group. - PubMed
-
- Spector TD, Da Silva JA. Pregnancy and rheumatoid arthritis: an overview. Am J Reprod Immunol. 1992;28:222–5. - PubMed
-
- Rabiah PK, Vitale AT. Noninfectious uveitis and pregnancy. Am J Ophthalmol. 2003;136:91–8. - PubMed
-
- Muller AF, Berghout A. Consequences of autoimmune thyroiditis before, during and after pregnancy. Minerva Endocrinol. 2003;28:247–54. - PubMed
-
- Chaouat G, Ledee-Bataille N, Dubanchet S, Zourbas S, Sandra O, Martal J. Reproductive immunology 2003: reassessing the Th1/Th2 paradigm? Immunol Lett. 2004;92:207–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
