

Use of recommended medications after myocardial infarction in Austria
- PMID: 18064529
- PMCID: PMC2249618
- DOI: 10.1007/s10654-007-9212-4
Use of recommended medications after myocardial infarction in Austria
Abstract
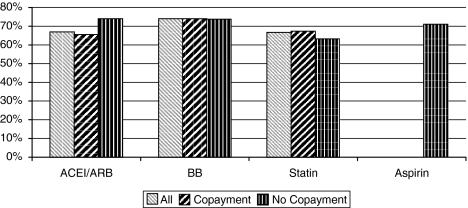
Guidelines recommend long-term use of beta-blockers (BB), statins, and angiotensin-converting-enzyme-inhibitors or angiotensin-receptor-blockers (ACEI/ARB) after myocardial infarction (MI), but data on their use after discharge are scarce. From Austrian sickness funds claims, we identified all acute MI patients who were discharged within 30 days and who survived >or=120 days after MI in 2004. We ascertained outpatient use of ACEI/ARBs, BBs, statins, and aspirin from all filled prescriptions between discharge and 120 days post MI. Comorbidities were ascertained from use of indicator drugs during the preceding year. Multivariate logistic regression was used to evaluate the independent determinants of study drug use. We evaluated 4,105 MI patients, whose mean age was 68.8 (+/-13.2) years; 59.5% were men. Within 120 days after MI, 67% filled prescriptions for ACE/ARBs, 74% for BBs, and 67% for statin. While 41% received all these classes and 34% two, 25% of patients received only one or none of these drugs. Older age and presence of severe mental illness were associated with lower use of all drug classes. Diabetics had greater ACEI/ARB use. Fewer BBs were used in patients with obstructive lung disease. Statin use was lower in patients using treatment for congestive heart failure (all P<0.001). We conclude that recommended medications were underused in Austrian MI survivors. Quality indicators should be established and interventions be implemented to ensure maximum secondary prevention after MI.
Figures
References
-
- Tunstall-Pedoe H, Kuulasmaa K, Mahonen M, Tolonen H, Ruokokoski E, Amouyel P. Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular disease. Lancet 1999;353:1547–57. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
