

Melatonin and bright-light treatment for rest-activity disruption in institutionalized patients with Alzheimer's disease
- PMID: 18070004
- PMCID: PMC2642966
- DOI: 10.1111/j.1532-5415.2007.01543.x
Melatonin and bright-light treatment for rest-activity disruption in institutionalized patients with Alzheimer's disease
Abstract
Objectives: To test whether the addition of melatonin to bright-light therapy enhances the efficacy in treating rest-activity (circadian) disruption in institutionalized patients with Alzheimer's disease (AD).
Design: Randomized, controlled trial.
Setting: Two nursing homes in San Francisco, California.
Participants: Fifty subjects (mean age 86) with AD.
Intervention: Experimental subjects received 1 hour of morning light exposure (> or = 2,500 lux in gaze direction) Monday to Friday for 10 weeks and 5 mg melatonin (LM, n=16) or placebo (LP, n=17) in the evening. Control subjects (n=17) received usual indoor light (150-200 lux).
Measurements: Nighttime sleep variables, day sleep time, day activity, day:night sleep ratio, and rest-activity parameters were determined using actigraphy.
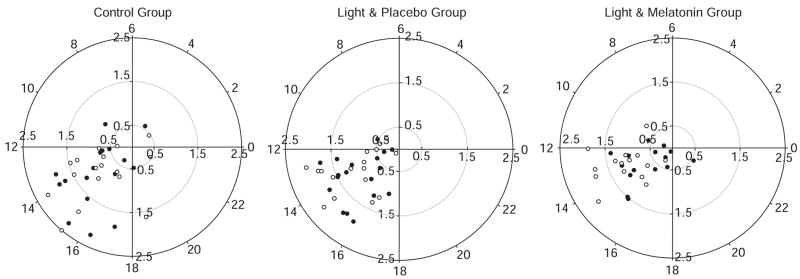
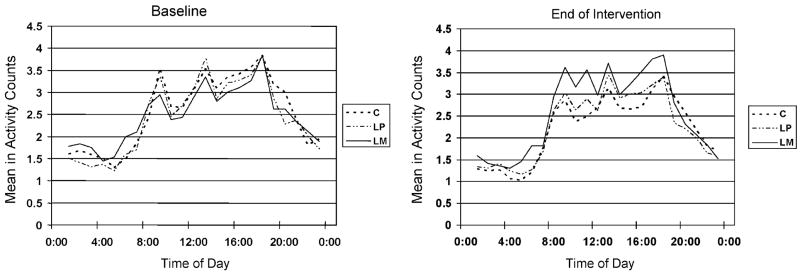
Results: Linear mixed models were employed to test the primary study hypotheses. No significant differences in nighttime sleep variables were found between groups. At the end of the intervention, the LM group showed significant improvement in daytime somnolence as indicated by a reduction in the duration of daytime sleep, an increase in daytime activity, and an improvement in day:night sleep ratio. The LM group also evidenced a significant increase in rest-activity rhythm amplitude and goodness of fit to the cosinor model.
Conclusion: Light treatment alone did not improve nighttime sleep, daytime wake, or rest-activity rhythm. Light treatment plus melatonin increased daytime wake time and activity levels and strengthened the rest-activity rhythm. Future studies should resolve the question of whether these improvements can be attributed to melatonin or whether the two zeitgebers interact to amplify efficacy.
Conflict of interest statement
Figures
References
-
- Yesavage JA, Friedman L, Ancoli-Israel S, et al. Development of diagnostic criteria for defining sleep disturbance in Alzheimer’s disease. J Geriatr Psychiatry Neurol. 2003;16:131–139. - PubMed
-
- McCurry SM, Ancoli-Israel S. Sleep dysfunction in Alzheimer’s disease and other dementias. Curr Treat Options Neurol. 2003;5:261–272. - PubMed
-
- Pollak CP, Perlick D. Sleep problems and institutionalization of the elderly. J Geriatr Psychiatry Neurol. 1991;4:204–210. - PubMed
-
- Hope T, Keene J, Gedling K, et al. Predictors of institutionalization for people with dementia living at home with a carer. Int J Geriatr Psychiatry. 1998;13:682–690. - PubMed
-
- Sullivan SC, Richards KC. Predictors of circadian sleep-wake rhythm maintenance in elders with dementia. Aging Ment Health. 2004;8:143–152. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
