

An evidence based alcohol screening, brief intervention and referral to treatment (SBIRT) curriculum for emergency department (ED) providers improves skills and utilization
- PMID: 18077305
- PMCID: PMC3976968
- DOI: 10.1300/J465v28n04_01
An evidence based alcohol screening, brief intervention and referral to treatment (SBIRT) curriculum for emergency department (ED) providers improves skills and utilization
Abstract
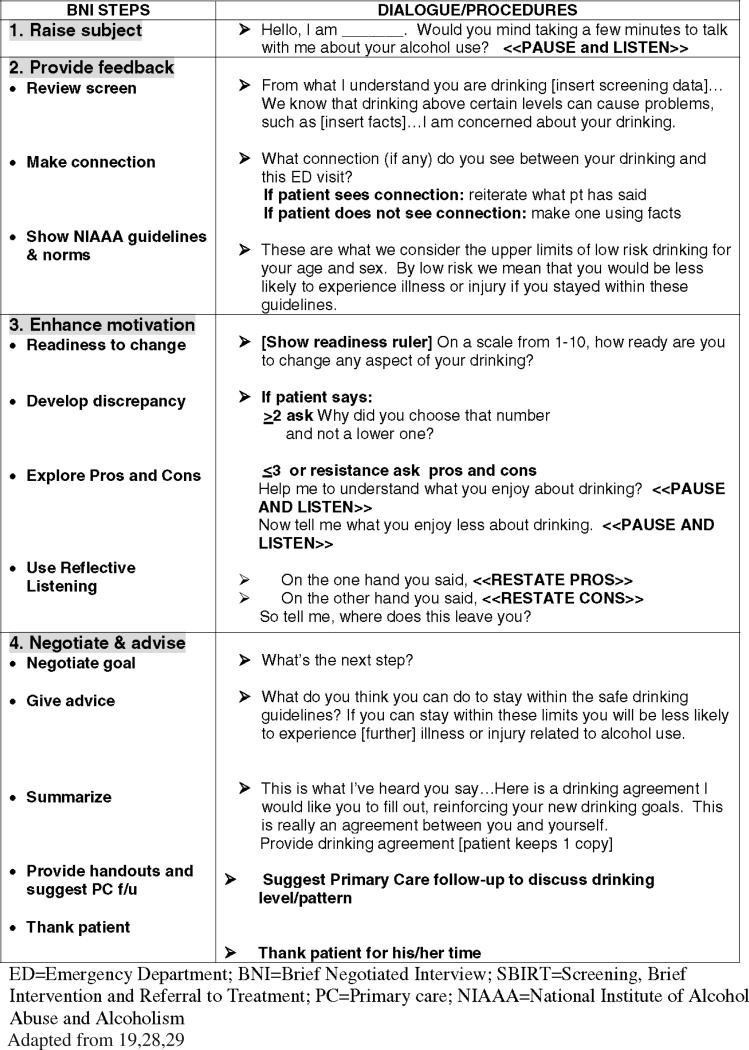
Objective: Emergency Departments (EDs) offer an opportunity to improve the care of patients with at-risk and dependent drinking by teaching staff to screen, perform brief intervention and refer to treatment (SBIRT). We describe here the implementation at 14 Academic EDs of a structured SBIRT curriculum to determine if this learning experience improves provider beliefs and practices.
Methods: ED faculty, residents, nurses, physician extenders, social workers, and Emergency Medical Technicians (EMTs) were surveyed prior to participating in either a two hour interactive workshops with case simulations, or a web-based program (www.ed.bmc.org/sbirt). A pre-post repeated measures design assessed changes in provider beliefs and practices at three and 12 months post-exposure.
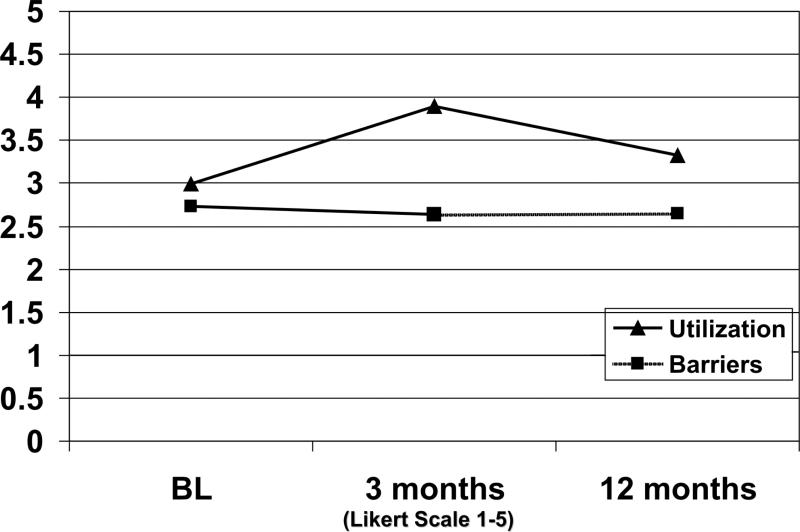
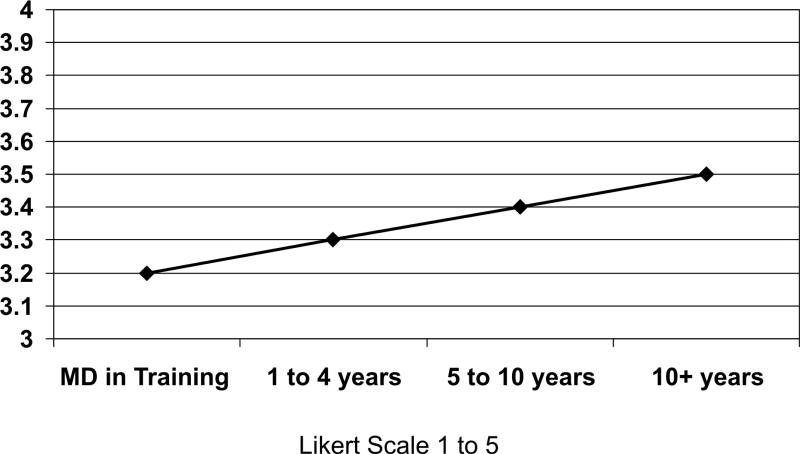
Results: Among 402 ED providers, 74% reported < 10 hours of prior professional alcohol-related education and 78% had < 2 hours exposure in the previous year. At 3-month follow-up, scores for self-reported confidence in ability, responsibility to intervene, and actual utilization of SBIRT skills all improved significantly over baseline. Gains decreased somewhat at 12 months, but remained above baseline. Length of time in practice was positively associated with SBIRT utilization, controlling for gender, race and type of profession. Persistent barriers included time limitations and lack of referral resources.
Conclusions: ED providers respond favorably to SBIRT. Changes in utilization were substantial at three months post-exposure to a standardized curriculum, but less apparent after 12 months. Booster sessions, trained assistants and infrastructure supports may be needed to sustain changes over the longer term.
Figures
References
-
- Harwood HJ. Updating estimates of economic costs of alcohol abuse in the United States: estimates, update methods, and data. National Institute of Alcohol Abuse and Alcoholism; Bethesda, MD: 2000.
-
- Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trend in DSM-IV alcohol abuse and dependence, 1991-1992 and 2001-2002. Drug Alcohol Depend. 2004;74:223–234. - PubMed
-
- Center for Disease Control Alcohol-attributable deaths and years of potential life lost–United States 2001, MMWR Morb Mort Wkly Rep. 2004;53:866–870. - PubMed
-
- Brewer RD, Swahn MH. Binge drinking and violence. JAMA. 2005;294:616–617. - PubMed
-
- McDonald AJ III, Wang N, Camargo CA., Jr US emergency department visits for alcohol-related diseases and injuries between 1992 and 2000. Arch Intern Med 2004. 164:531–537. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
