

Impact of collateral flow on tissue fate in acute ischaemic stroke
- PMID: 18077482
- PMCID: PMC2702489
- DOI: 10.1136/jnnp.2007.132100
Impact of collateral flow on tissue fate in acute ischaemic stroke
Abstract
Background: Collaterals may sustain penumbra prior to recanalisation yet the influence of baseline collateral flow on infarct growth following endovascular therapy remains unknown.
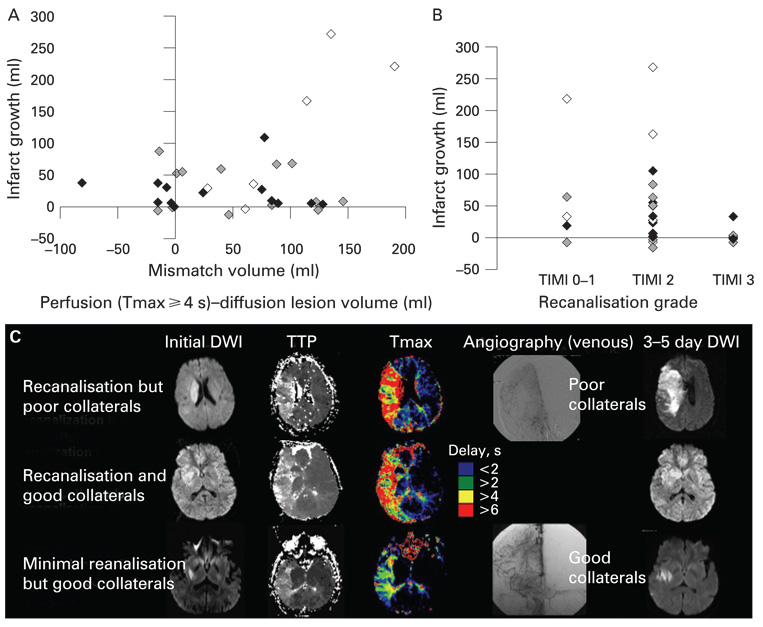
Methods: Consecutive patients underwent serial diffusion and perfusion MRI before and after endovascular therapy for acute cerebral ischaemia. We assessed the relationship between MRI diffusion and perfusion lesion indices, angiographic collateral grade and infarct growth. Tmax perfusion lesion maps were generated and diffusion-perfusion mismatch regions were divided into Tmax >or=4 s (severe delay) and Tmax >or=2 but <4 s (mild delay).
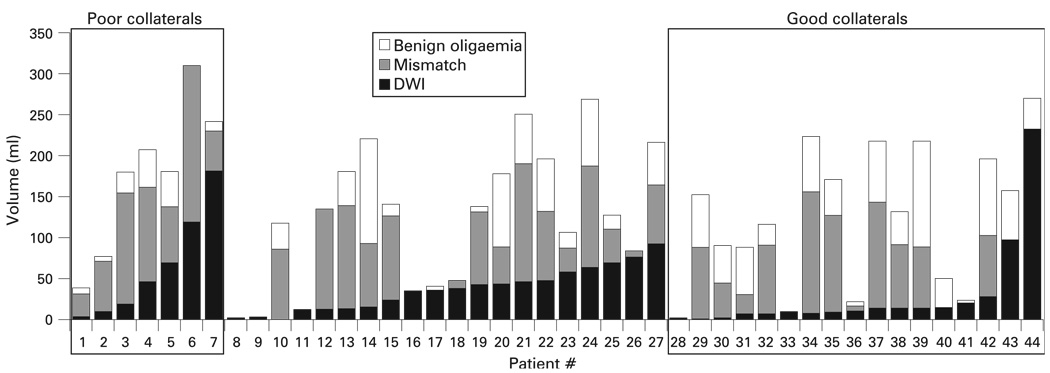
Results: Among 44 patients, collateral grade was poor in 7 (15.9%), intermediate in 20 (45.5%) and good in 17 (38.6%) patients. Although diffusion-perfusion mismatch volume was not different depending on the collateral grade, patients with good collaterals had larger areas of milder perfusion delay than those with poor collaterals (p = 0.005). Among 32 patients who underwent day 3-5 post-treatment MRIs, the degree of pretreatment collateral circulation (r = -0.476, p = 0.006) and volume of diffusion-perfusion mismatch (r = 0.371, p = 0.037) were correlated with infarct growth. Greatest infarct growth occurred in patients with both non-recanalisation and poor collaterals. Multiple regression analysis revealed that pretreatment collateral grade was independently associated with infarct growth.
Conclusion: Our data suggest that angiographic collateral grade and penumbral volume interactively shape tissue fate in patients undergoing endovascular recanalisation therapy. These angiographic and MRI parameters provide complementary information about residual blood flow that may help guide treatment decision making in acute cerebral ischaemia.
Figures
Comment in
-
Collateral damage in acute stroke treatment: a new role for an old concept?J Neurol Neurosurg Psychiatry. 2008 Jun;79(6):615-6. doi: 10.1136/jnnp.2007.140525. J Neurol Neurosurg Psychiatry. 2008. PMID: 18487551 No abstract available.
References
-
- Hjort N, Butcher K, Davis SM, et al. Magnetic resonance imaging criteria for thrombolysis in acute cerebral infarct. Stroke. 2005;36:388–397. - PubMed
-
- Kohrmann M, Juttler E, Fiebach JB, et al. MRI versus CT-based thrombolysis treatment within and beyond the 3 h time window after stroke onset: A cohort study. Lancet Neurol. 2006;5:661–667. - PubMed
-
- Powers WJ. Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol. 1991;29:231–240. - PubMed
-
- Liebeskind DS. Collateral circulation. Stroke. 2003;34:2279–2284. - PubMed
-
- Liebeskind DS. Collaterals in acute stroke: Beyond the clot. Neuroimaging Clin N Am. 2005;15:553–573. x. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources