

Cervical human papillomavirus (HPV) infection and HPV type 16 antibodies in South African women
- PMID: 18077644
- PMCID: PMC2238115
- DOI: 10.1128/JCM.01322-07
Cervical human papillomavirus (HPV) infection and HPV type 16 antibodies in South African women
Abstract
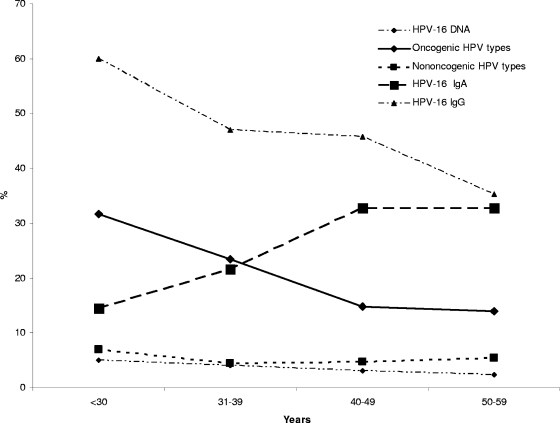
There is a high incidence of cervical cancer in South African women. No large studies to assess human papillomavirus virus (HPV) infection or HPV type 16 (HPV-16) exposure have occurred in the region, a requirement for policy making with regards to HPV screening and the introduction of vaccines. Control women (n = 1,003) enrolled in a case control study of hormonal contraceptives and cervical cancer were tested for 27 cervical HPV types by reverse line blot analysis. The seroprevalence of HPV-16 immunoglobulin G (IgG) and IgA antibodies was assessed by a virus-like particle-based enzyme-linked immunoassay of 908 and 904 control women, respectively, and of 474 women with cervical cancer. The cervical HPV prevalence was 26.1%. The HPV-16 IgG seroprevalence was 44.4% and the HPV-16 IgA seroprevalence was 28.7% in control women, and these levels were significantly higher (61.8% and 52.7%, respectively) for women with cervical cancer (odds ratio [OR], 2.1 and 2.8, respectively). The cervical HPV prevalence showed an association with cervical disease, and the HPV-16 IgG prevalence decreased while the HPV-16 IgA prevalence increased with increasing age (P < 0.05). The prevalence of oncogenic HPV types (including HPV-16) decreased with age, whereas nononcogenic HPV types showed limited association with age. Multivariate analysis revealed cervical HPV infection to be associated with herpes simplex virus type 2 infection (OR, 1.7) and increasing years of education (OR, 1.9). HPV-16 IgG antibodies were inversely associated with current smoking status (OR, 0.6), and the presence of HPV-16 IgA antibodies was inversely associated with the use of alcohol (OR, 2.1) and inversely associated with the use of oral contraceptives (OR, 0.6). High levels of exposure to HPV, and particularly HPV-16, were evident in this population. The apparent increase of serum HPV-16 IgA with increasing age requires further investigation.
Figures
References
-
- Allan, B. R., D. J. Marais, L. Denny, M. Hoffman, S. Shapiro, and A. L. Williamson. 2006. The agreement between cervical abnormalities identified by cytology and detection of high-risk types of human papillomavirus. S. Afr. Med. J. 961186-1190. - PubMed
-
- Bontkes, H. J., T. D. de Gruijl, J. M. Walboomers, J. T. Schiller, J. Dillner, T. J. Helmerhorst, R. H. Verheijen, R. J. Scheper, and C. J. Meijer. 1999. Immune responses against human papillomavirus (HPV) type 16 virus-like particles in a cohort study of women with cervical intraepithelial neoplasia. II. Systemic but not local IgA responses correlate with clearance of HPV-16. J. Gen. Virol. 80409-417. - PubMed
-
- Bosch, F. X., M. M. Manos, N. Munoz, M. Sherman, A. M. Jansen, J. Peto, M. H. Schiffman, V. Moreno, R. Kurman, K. V. Shah, et al. 1995. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. J. Natl. Cancer Inst. 87796-802. - PubMed
-
- Burchell, A. N., R. L. Winer, S. S. de Sanjose, and E. L. Franco. 2006. Epidemiology and transmission dynamics of genital HPV infection. Vaccine 24(Suppl. 3)S52-S61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
