

Clinical use of recombinant human activated factor VII (rFVIIa) in the prevention and treatment of bleeding episodes in patients with Glanzmann's thrombasthenia
- PMID: 18078017
- PMCID: PMC2291310
Clinical use of recombinant human activated factor VII (rFVIIa) in the prevention and treatment of bleeding episodes in patients with Glanzmann's thrombasthenia
Abstract
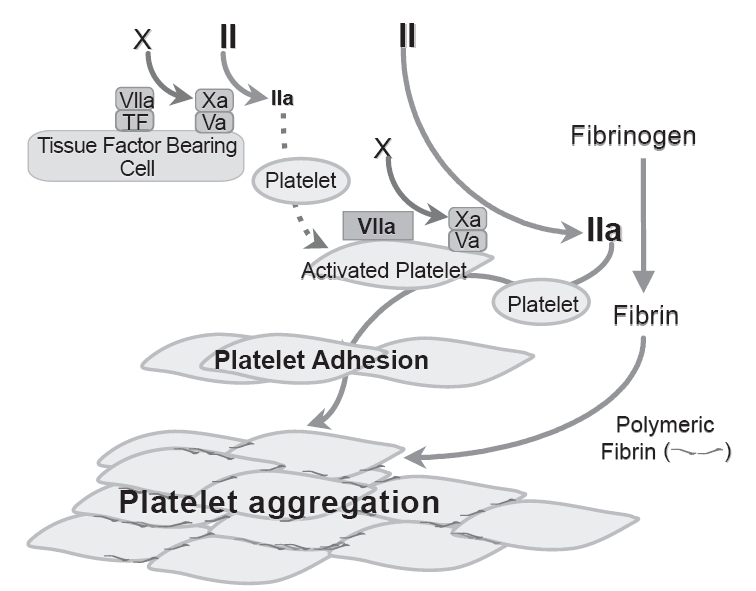
Glanzmann's thrombasthenia (GT) is a congenital qualitative platelet disorders due to the deficiency or defect of platelet membrane GPIIb/IIIa (integrin alpha(IIb)beta3). The standard treatment for bleeding is platelet transfusion but repeated transfusion may result in the development of anti-platelet antibodies (to HLA and/or GPlIbIIIa) rendering future platelet transfusion ineffective. Alternative effective agent(s) are needed. There are increasing reports documenting efficacy of high dose rFVIIa in GT patients with adverse events uncommon. The efficacy is supported by evidence that high concentration FVIIa binds to activated platelet surface and improves thrombin generation to enhance deposition (adhesion) and aggregation of platelets lacking GPIIb/IIIa. While there are increasing clinical experiences, evidence-based clinical data are not available. There is a need for more clinical studies, particularly clinical trials, to further assess the efficacy, safety (particularly thrombotic events) and optimal regimen ofrFVIIa in GT patients, either singly or in combination with other hemostatic agents such as platelet transfusion. In the absence of this data, for treatment of severe bleeding in GT patients with platelet antibodies and platelet refractoriness, rFVIIa at dose 90 microg/kg every 2 h for 3 or more doses could be considered. This more "optimal regimen" derived from a recent International Survey needs confirmation with larger studies. What the optimal regimen for surgical coverage is remains unresolved.
Figures
References
-
- Abshire T, Kenet G. Recombinant factor VIIa: review of efficacy, dosing regimens and safety in patients with congenital and acquired factor VIII or IX inhibitors. J Thromb Haemost. 2004;2:899–909. - PubMed
-
- Aledort LM. Comparative thrombotic event incidence after infusion of recombinant factor VIIa versus factor VIII inhibitor bypass activity. J Thromb Haemost. 2004;2:1700–08. - PubMed
-
- Almeida AM, Khair K, Hann I, et al. The use of recombinant factor VIIa in children with inherited platelet function disorders. Br J Haematol. 2003;121:477–81. - PubMed
-
- Bell JA, Savidge GF. Glanzmann’s thrombasthenia proposed optimal management during surgery and delivery. Clin Appl Thromb Hemost. 2003;9:167–70. - PubMed
-
- Berrettini M, Mariani G, Schiavoni M, et al. Pharmacokinetic evaluation of recombinant, activated factor VII in patients with inherited factor VII deficiency. Haematologica. 2001;86:640–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
