

Catheter angiography, MR angiography, and MR perfusion in posterior reversible encephalopathy syndrome
- PMID: 18079186
- PMCID: PMC8118858
- DOI: 10.3174/ajnr.A0839
Catheter angiography, MR angiography, and MR perfusion in posterior reversible encephalopathy syndrome
Abstract
Background and purpose: The cause of posterior reversible encephalopathy syndrome (PRES) is unknown. Two primary hypotheses exist: 1) hypertension exceeding auto-regulatory limits leading to forced hyper-perfusion and 2) vasoconstriction and hypo-perfusion leading to ischemia with resultant edema. The purpose of this study was to evaluate the catheter angiography (CA), MR angiography (MRA), and MR perfusion (MRP) features in PRES in order to render further insight into its mechanism of origin.
Materials and methods: In 47 patients with PRES, 9 CAs and 43 MRAs were evaluated for evidence of vasculopathy (vasoconstriction and vasodilation), and 15 MRP studies were evaluated for altered relative cerebral blood volume (rCBV) in PRES lesions and regions. Visualization of vessels on MRA and toxicity blood pressures were compared with the extent of hemispheric vasogenic edema.
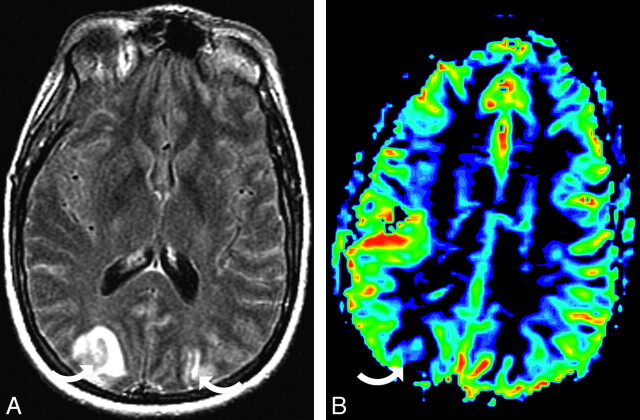
Results: Vasculopathy was present in 8 of 9 patients on CA (direct correlation to MRA in 3/6 patients). At MRA, moderate to severe vessel irregularity consistent with vasoconstriction and vasodilation was present in 30 of 43 patients and vessel pruning or irregularity in 7 patients, with follow-up MRA demonstrating reversal of vasoconstriction or vasodilation in 9 of 11 patients. Vasogenic edema was less in patients with hypertension compared with patients who were normotensive. Preserved normal length of the posterior cerebral artery (PCA) was commonly seen in patients with severe hypertension despite diffuse or focal vasoconstriction or vasodilation. In these patients, lengthier visualization of the distal PCA correlated with a lower grade of hemispheric edema (P = .002). Cortical rCBV was significantly reduced in 51 of 59 PRES lesions and regions compared with a healthy reference cortex (average 61% of reference cortex) with mild decrease in the remainder.
Conclusion: Vasculopathy was a common finding on CA and MRA in our patients with PRES, and MRP demonstrated reduced cortical rCBV in PRES lesions. Vasogenic edema was reduced in patients with hypertension, and superior distal PCA visualization correlated with reduced hemispheric edema in patients with PRES and severe hypertension.
Figures





Comment in
-
Catheter angiography, MR angiography, and MR perfusion in posterior reversible encephalopathy syndrome.AJNR Am J Neuroradiol. 2009 Feb;30(2):E19; author reply E20. doi: 10.3174/ajnr.A1285. AJNR Am J Neuroradiol. 2009. PMID: 19208904 Free PMC article. No abstract available.
References
-
- Raroque HG, Orrison WW, Rosenberg GA. Neurologic involvement in toxemia of pregnancy: reversible MRI lesions. Neuroradiology 1990;40:167–69 - PubMed
-
- Bartynski WS, Grabb BC, Zeigler Z, et al. Watershed imaging features and clinical vascular injury in cyclosporin A neurotoxicity. J Comput Assist Tomogr 1997;21:872–80 - PubMed
-
- Schaefer PW, Buonanno FS, Gonzalez RG, et al. Diffusion-weighted imaging discriminates between cytotoxic and vasogenic edema in a patient with eclampsia. Stroke 1997;28:1082–85 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical