

Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise)
- PMID: 18082522
- PMCID: PMC2190779
- DOI: 10.1016/j.amjcard.2007.07.027
Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise)
Abstract
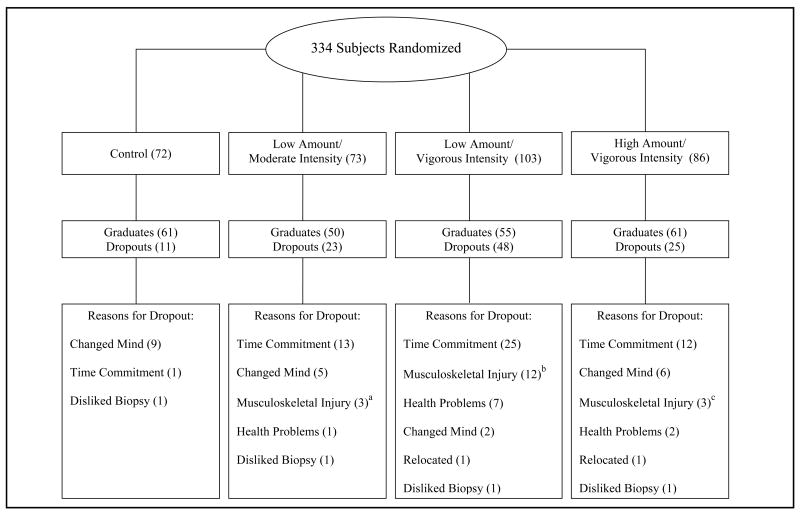
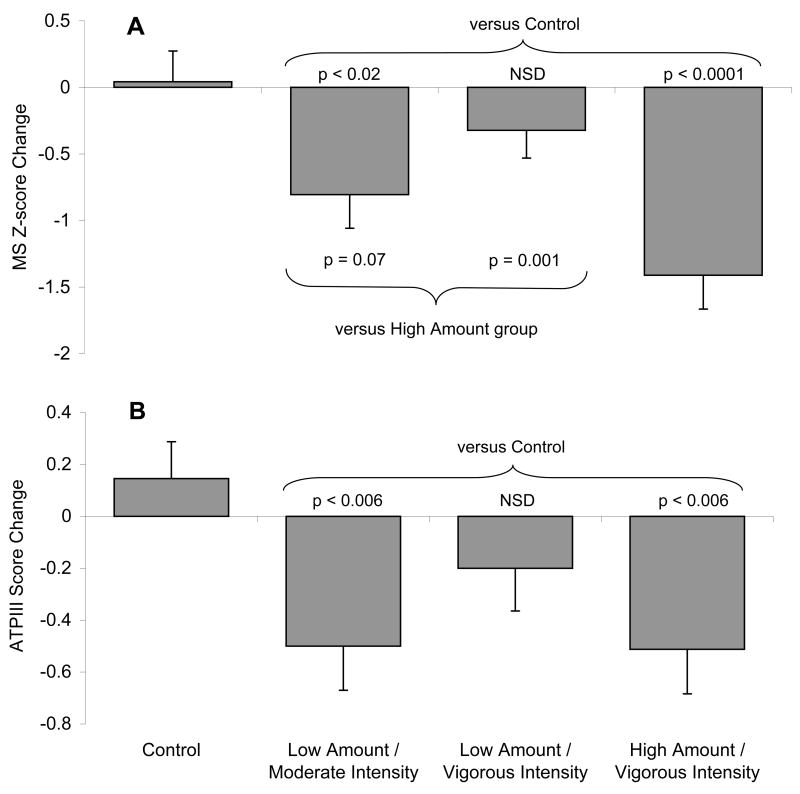
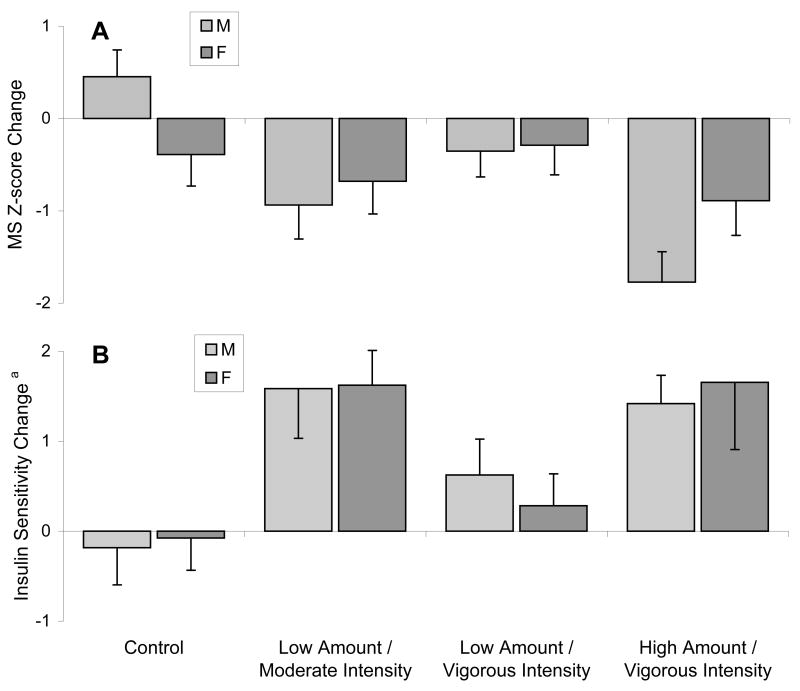
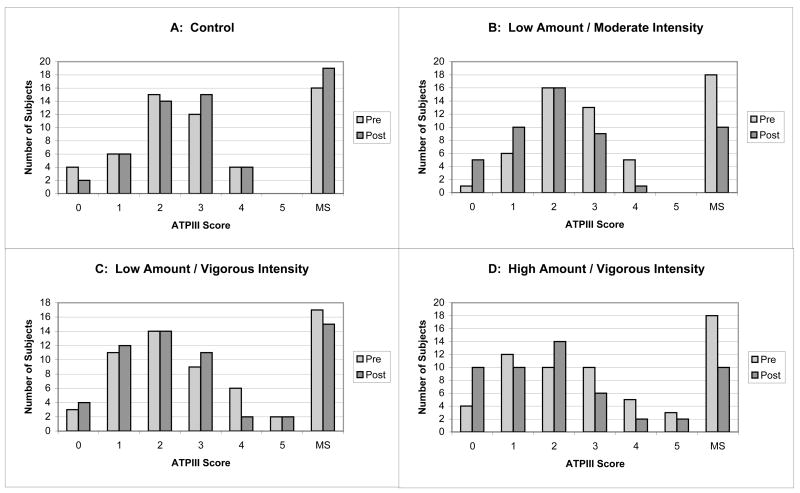
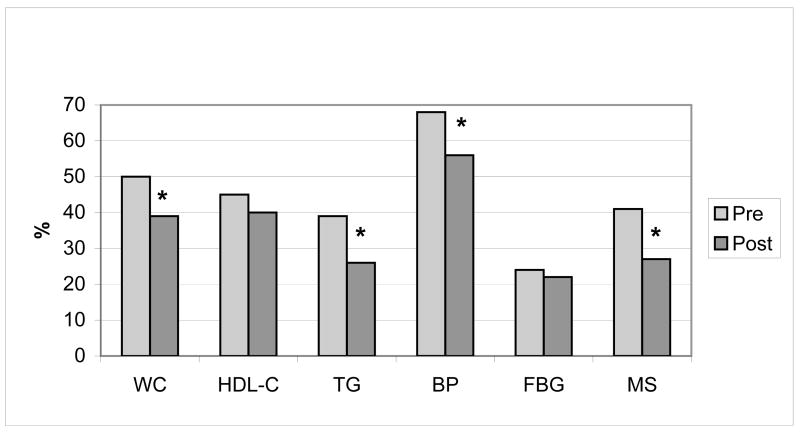
Although exercise improves individual risk factors for metabolic syndrome (MS), there is little research on the effect of exercise on MS as a whole. The objective of this study was to determine how much exercise is recommended to decrease the prevalence of MS. Of 334 subjects randomly assigned, 227 finished and 171 (80 women, 91 men) had complete data for all 5 Adult Treatment Panel III-defined MS risk factors and were included in this analysis. Subjects were randomly assigned to a 6-month control or 1 of 3 eight-month exercise training groups of (1) low amount/moderate intensity (equivalent to walking approximately 19 km/week), (2) low amount/vigorous intensity (equivalent to jogging approximately 19 km/week), or (3) high amount/vigorous intensity (equivalent to jogging approximately 32 km/week). The low-amount/moderate-intensity exercise prescription improved MS relative to inactive controls (p <0.05). However, the same amount of exercise at vigorous intensity was not significantly better than inactive controls, suggesting that lower-intensity exercise may be more effective in improving MS. The high-amount/vigorous-intensity group improved MS relative to controls (p <0.0001), the low-amount/vigorous-intensity group (p = 0.001), and the moderate-intensity group (p = 0.07), suggesting an exercise-dose effect. In conclusion, a modest amount of moderate-intensity exercise in the absence of dietary changes significantly improved MS and thus supported the recommendation that adults get 30 minutes of moderate-intensity exercise every day. A higher amount of vigorous exercise had greater and more widespread benefits. Finally, there was an indication that moderate-intensity may be better than vigorous-intensity exercise for improving MS.
Figures
References
-
- Panel E. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–2497. - PubMed
-
- Kraus W, Torgan C, Duscha B, Norris J, Brown S, Cobb F, Bales C, Annex B, Samsa G, Houmard J, Slentz C. Studies of a targeted risk reduction intervention through defined exercise. Med Sci Sports Exerc. 2001;33:1774–1784. - PubMed
-
- Otvos J, Jeyarajah E, Bennett D, Krauss R. Development of a proton nuclear magnetic resonance spectroscopic method for determining plasma lipoprotein concentrations and subspecies distributions from a single, rapid measurement. Clin Chem. 1992;38:1632–1638. - PubMed
-
- Bergman R, Finegood D, Ader M. Assessment of insulin sensitivity in vivo. Endocrine Reviews. 1985;6:45–86. - PubMed
-
- Grundy S, Cleeman J, Daniels S, Donato K, Eckel R, Franklin B, Gordon D, Krauss R, Savage P, Smith S, Spertus J, Costa F. Diagnosis and management of the metabolic syndrome: an AHA/NHLBI scientific statement. Circulation. 2005;112:2735–2752. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
