

Clinical utility of laser-Doppler vibrometer measurements in live normal and pathologic human ears
- PMID: 18091103
- PMCID: PMC2572196
- DOI: 10.1097/AUD.0b013e31815d63a5
Clinical utility of laser-Doppler vibrometer measurements in live normal and pathologic human ears
Abstract
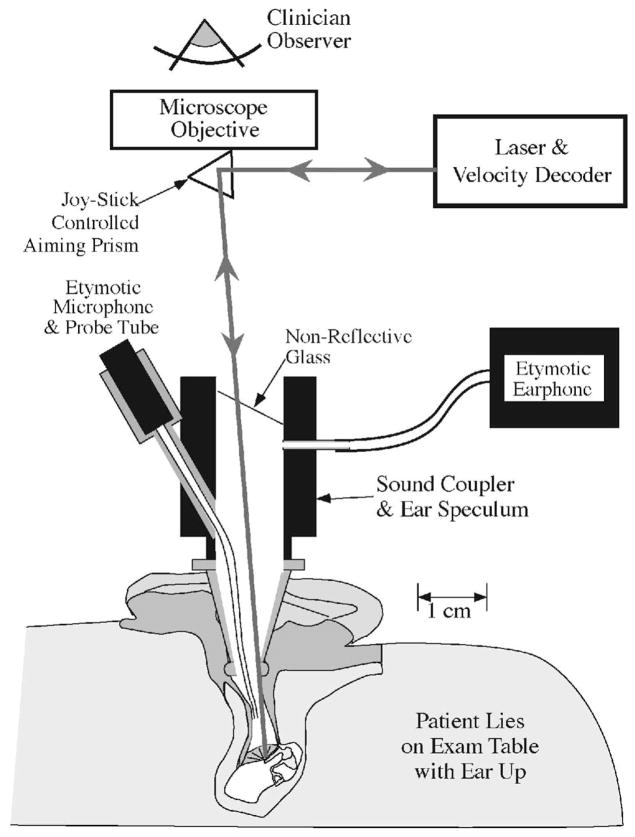
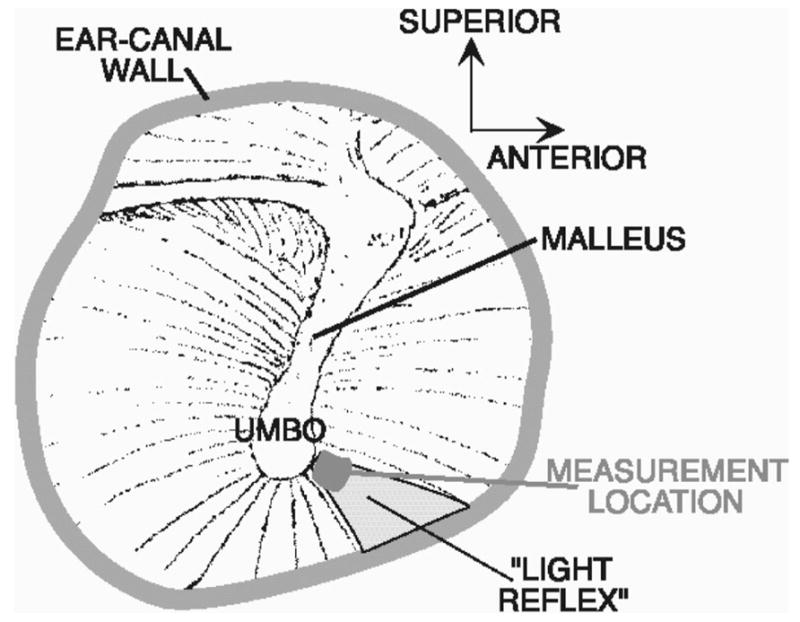
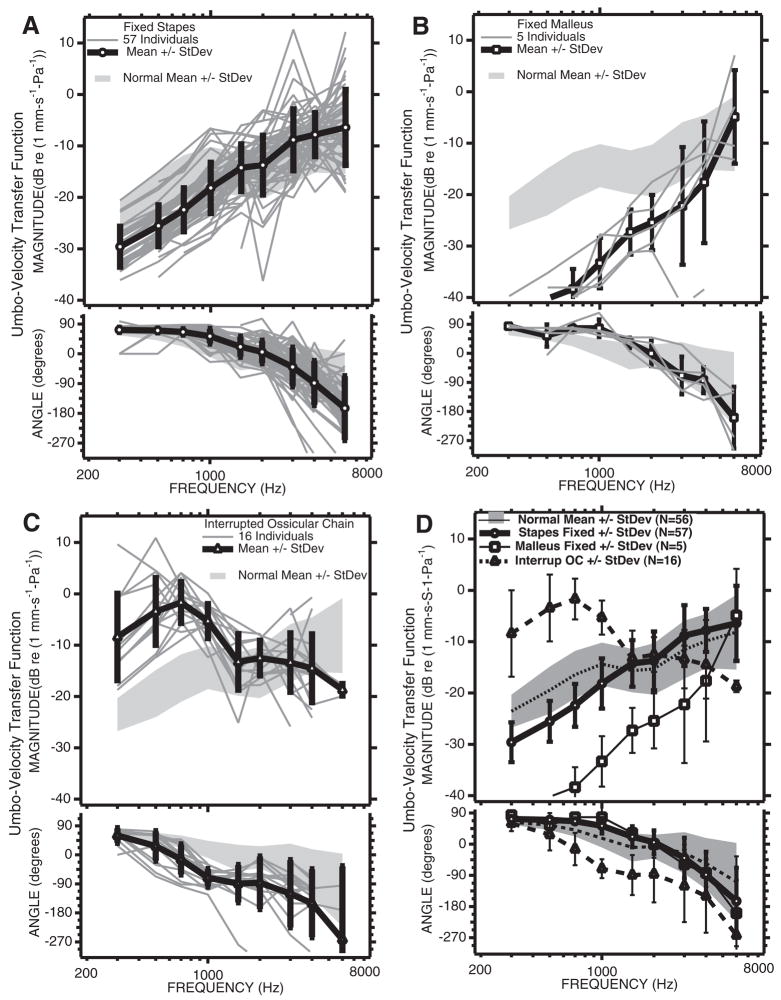
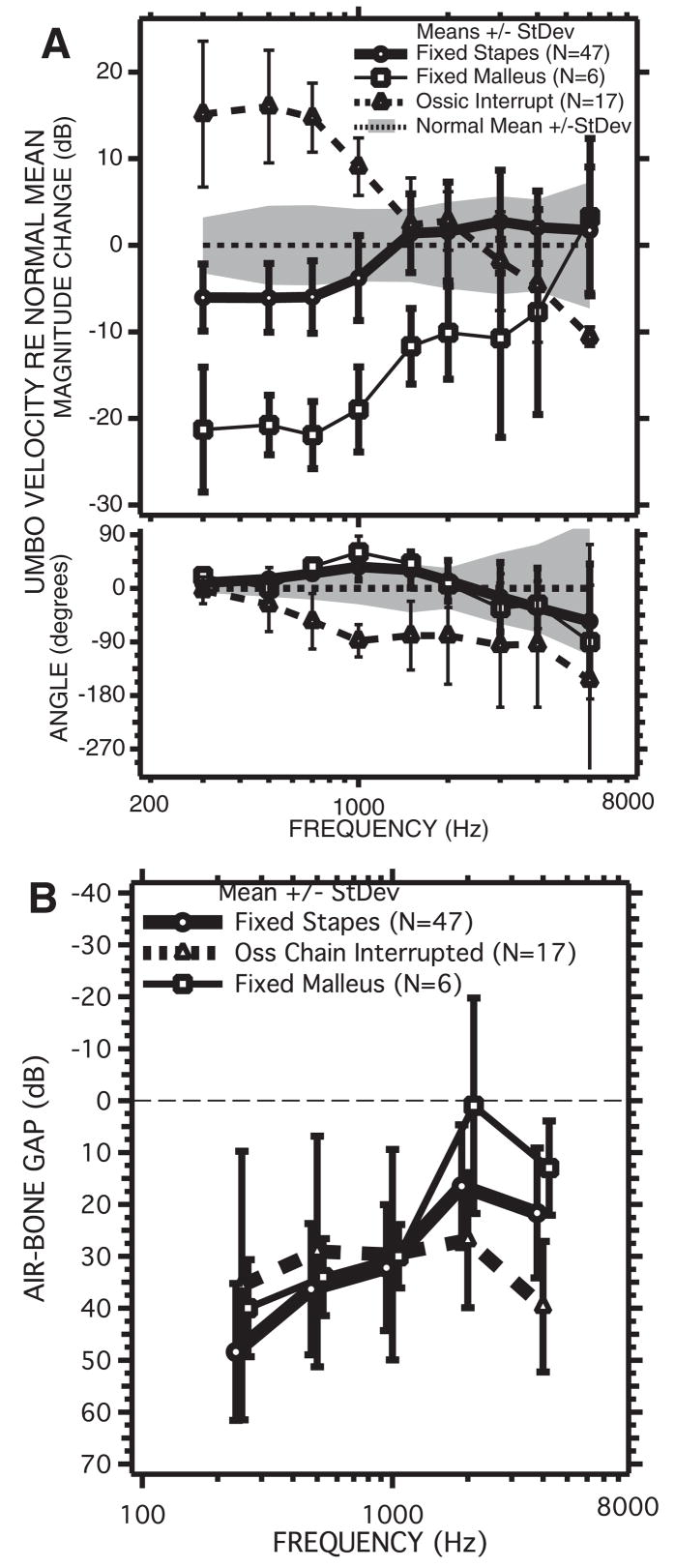
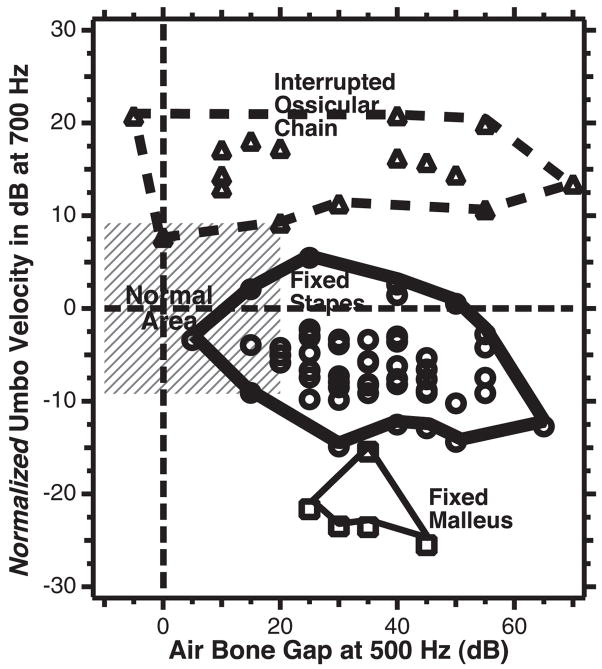
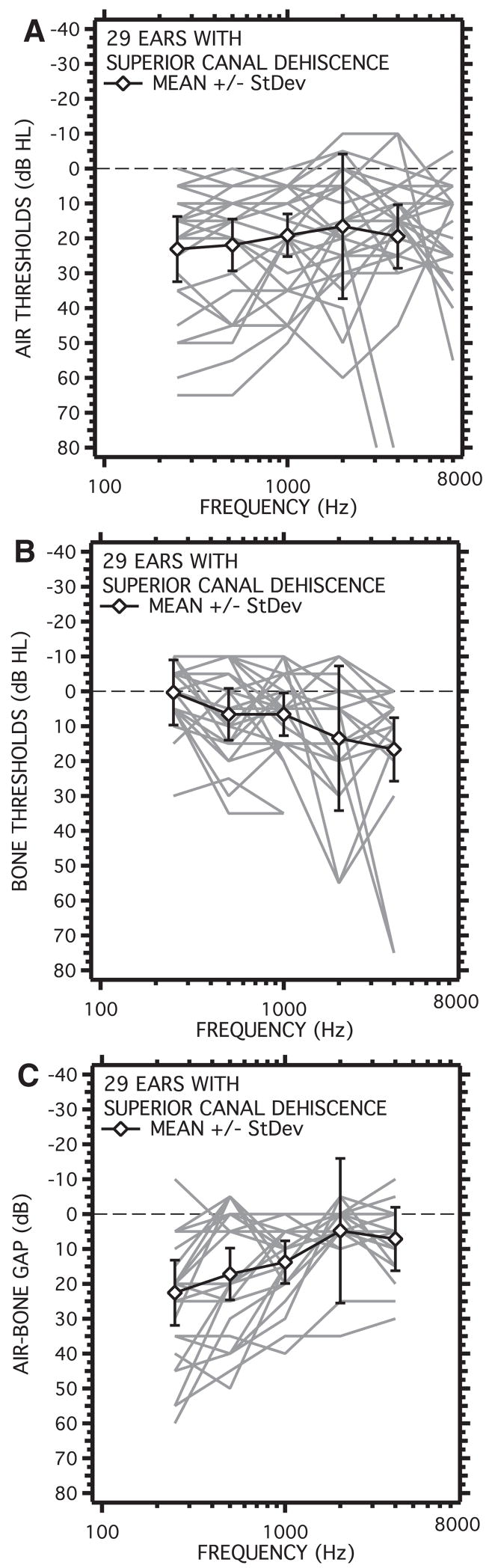
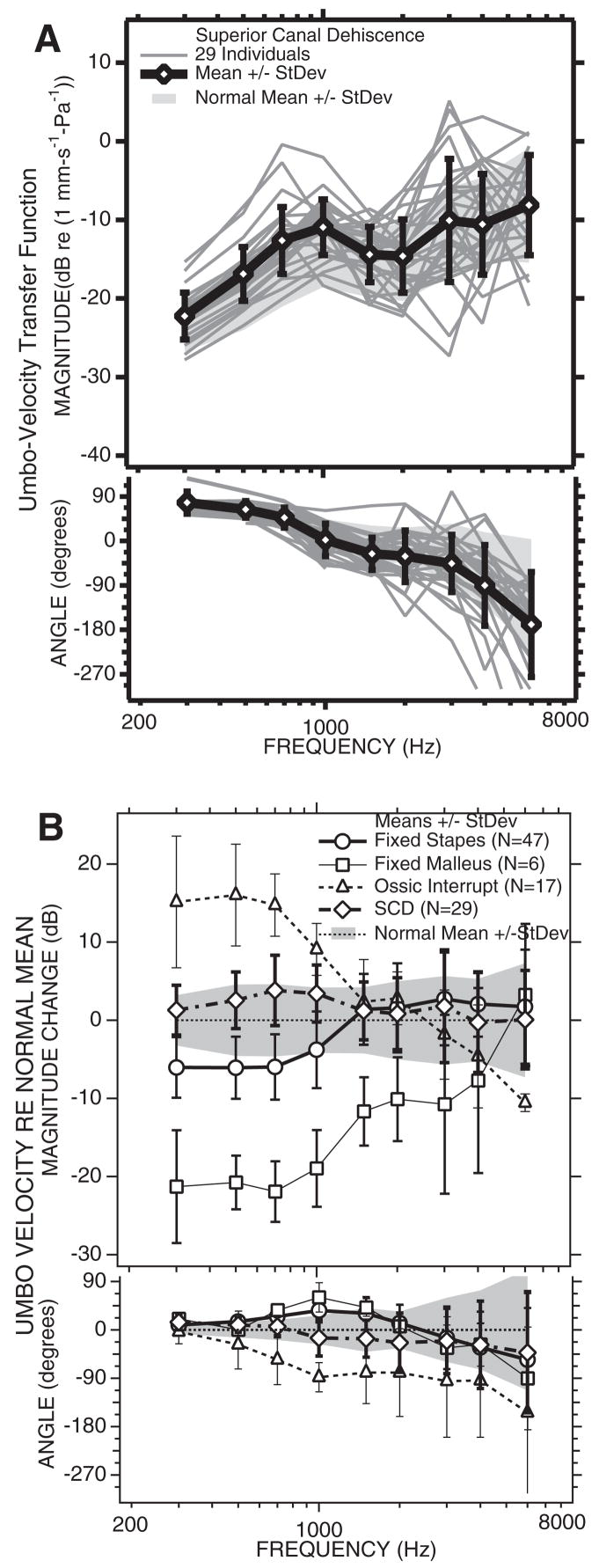
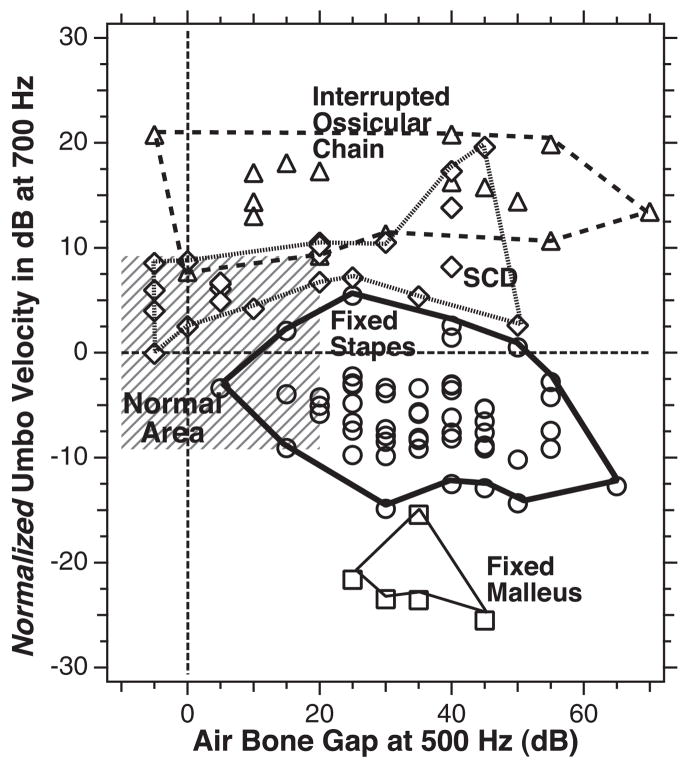
The laser-Doppler vibrometer (LDV) is a research tool that can be used to quickly measure the sound-induced velocity of the tympanic membrane near the umbo (the inferior tip of the malleus) in live human subjects and patients. In this manuscript we demonstrate the LDV to be a sensitive and selective tool for the diagnosis and differentiation of various ossicular disorders in patients with intact tympanic membranes and aerated middle ears. Patients with partial or total ossicular interruption or malleus fixation are readily separated from normal-hearing subjects with the LDV. The combination of LDV measurements and air-bone gap can distinguish patients with fixed stapes from those with normal ears. LDV measurements can also help differentiate air-bone gaps produced by ossicular pathologies from those associated with pathologies of inner-ear sound conduction such as a superior semicircular canal dehiscence.
Figures
References
-
- Allen JB. Measurements of eardrum acoustic impedance. In: Allen JB, Hall JL, Hubbard A, Neely ST, Tubis A, editors. Peripheral auditory mechanisms. New York: Springer-Verlag; 1986. pp. 44–51.
-
- Brantberg K, Bergenius J, Mendel L, Witt H, Tribukait A, Ygge J. Symptoms, findings and treatment in patients with dehiscence of the superior semicircular canal. Acta Otolaryngologica. 2001;121:68–75. - PubMed
-
- Brantberg K, Löfqvist L, Fransson PA. Large vestibular evoked myogenic potentials in response to bone-conducted sound in patients with superior canal dehiscence syndrome. Audiology and Neuro-Otology. 2004;9:173–182. - PubMed
-
- Carhart R. Bone conduction advances following fenestration surgery. Transactions of the American Academy of Opthamology and Otolaryngology. 1952;56:621–629. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
