

Evaluation of neurologic deficit without apparent cause: the importance of a multidisciplinary approach
- PMID: 18092568
- PMCID: PMC2141729
- DOI: 10.1080/10790268.2007.11754585
Evaluation of neurologic deficit without apparent cause: the importance of a multidisciplinary approach
Abstract
Background/objective: A patient presenting with an acute neurologic deficit with no apparent etiology presents a diagnostic dilemma. A broad differential diagnosis must be entertained, considering both organic and psychiatric causes.
Methods: A case report and thorough literature review of acute paraplegia after a low-energy trauma without a discernible organic etiology.
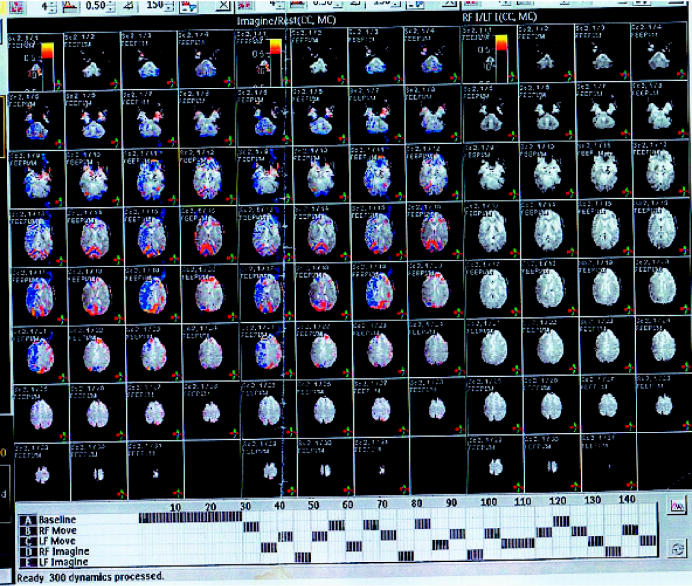
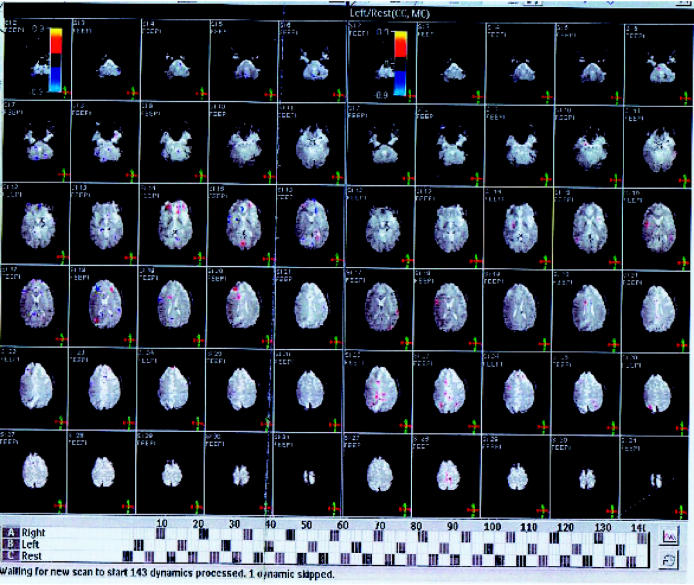
Results: Diagnostic imaging excluded any bony malalignment or fracture and any abnormality on magnetic resonance imaging. When no organic etiology was identified, a multidisciplinary approach using neurology, psychiatry, and physical medicine and rehabilitation services was applied. Neurophysiologic testing confirmed the absence of an organic disorder, and at this juncture, diagnostic efforts focused on identifying any psychiatric disorder to facilitate appropriate treatment for this individual. The final diagnosis was malingering.
Conclusions: The full psychiatric differential diagnosis should be considered in the evaluation of any patient with an atypical presentation of paralysis. A thorough clinical examination in combination with the appropriate diagnostic studies can confidently exclude an organic disorder. When considering a psychiatric disorder, the differential diagnosis should include conversion disorder and malingering, although each must remain a diagnosis of exclusion. Maintaining a broad differential diagnosis and involving multiple disciplines (neurology, psychiatry, social work, medical specialists) early in the evaluation of atypical paralysis may facilitate earlier diagnosis and initiation of treatment for the underlying etiology.
Figures
References
-
- Borock EC, Gabram SG, Jacobs LM, Murphy MA. A prospective analysis of a two-year experience using computed tomography as an adjunct for cervical spine clearance. J Trauma. 1991;31:1001–1005. - PubMed
-
- Esce PG, Haines SJ. Acute treatment of spinal cord injury. Curr Treat Options Neurol. 2000;2:517–524. - PubMed
-
- Miglietta MA, Levins T, Robb TV. Evaluation of spine injury in blunt trauma. J Am Osteopath Assoc. 2002;102:87–91. - PubMed
-
- American Psychiatric Association. Task Force on DSM-IV. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR. 4th ed. Washington, DC: American Psychiatric Association; 2000. text revision.
-
- Watson D, Pennebaker JW. Health complaints, stress, and distress: exploring the central role of negative affectivity. Psychol Rev. 1989;96:234–254. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical