

The contribution of teleconsultation and videoconferencing to diabetes care: a systematic literature review
- PMID: 18093904
- PMCID: PMC2270420
- DOI: 10.2196/jmir.9.5.e37
The contribution of teleconsultation and videoconferencing to diabetes care: a systematic literature review
Abstract
Background: A systematic literature review was carried out to study the benefits of teleconsultation and videoconferencing on the multifaceted process of diabetes care. Previous reviews focused primarily on usability of technology and considered mainly one-sided interventions.
Objective: The objective was to determine the benefits and deficiencies of teleconsultation and videoconferencing regarding clinical, behavioral, and care coordination outcomes of diabetes care.
Methods: Electronic databases (Medline, PiCarta, PsycINFO, ScienceDirect, Telemedicine Information Exchange, ISI Web of Science, Google Scholar) were searched for relevant publications. The contribution to diabetes care was examined for clinical outcomes (eg, HbA(1c), blood pressure, quality of life), behavioral outcomes (patient-caregiver interaction, self-care), and care coordination outcomes (usability of technology, cost-effectiveness, transparency of guidelines, equity of care access). Randomized controlled trials (RCTs) with HbA(1c) as an outcome were pooled using standard meta-analytical methods.
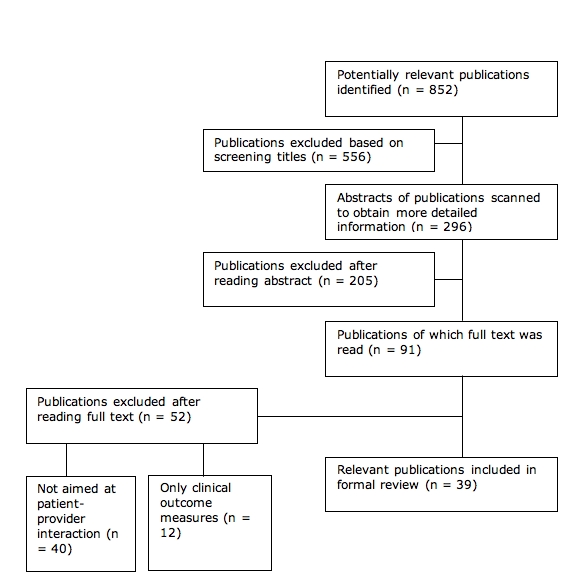
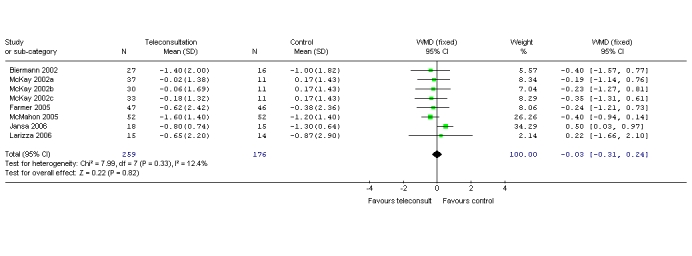
Results: Of 852 publications identified, 39 met the inclusion criteria for electronic communication between (groups of) caregivers and patients with type 1, type 2, or gestational diabetes. Studies that evaluated teleconsultation or videoconferencing not particularly aimed at diabetes were excluded, as were those that described interventions aimed solely at clinical improvements (eg, HbA(1c)). There were 22 interventions related to teleconsultation, 13 to videoconferencing, and 4 to combined teleconsultation and videoconferencing. The heterogeneous nature of the identified videoconferencing studies did not permit a formal meta-analysis. Pooled results from the six RCTs of the identified teleconsultation studies did not show a significant reduction in HbA(1c) (0.03%, 95% CI = - 0.31% to 0.24%) compared to usual care. There was no significant statistical heterogeneity among the pooled RCTs (chi(2) (7)= 7.99, P = .33). It can be concluded that in the period under review (1994-2006) 39 studies had a scope broader than clinical outcomes and involved interventions allowing patient-caregiver interaction. Most of the reported improvements concerned satisfaction with technology (26/39 studies), improved metabolic control (21/39), and cost reductions (16/39). Improvements in quality of life (6/39 studies), transparency (5/39), and better access to care (4/39) were hardly observed. Teleconsultation programs involving daily monitoring of clinical data, education, and personal feedback proved to be most successful in realizing behavioral change and reducing costs. The benefits of videoconferencing were mainly related to its effects on socioeconomic factors such as education and cost reduction, but also on monitoring disease. Additionally, videoconferencing seemed to maintain quality of care while producing cost savings.
Conclusions: The selected studies suggest that both teleconsultation and videoconferencing are practical, cost-effective, and reliable ways of delivering a worthwhile health care service to diabetics. However, the diversity in study design and reported findings makes a strong conclusion premature. To further the contribution of technology to diabetes care, interactive systems should be developed that integrate monitoring and personalized feedback functions.
Conflict of interest statement
None declared.
Figures
References
-
- Ouwens Marielle, Wollersheim Hub, Hermens Rosella, Hulscher Marlies, Grol Richard. Integrated care programmes for chronically ill patients: a review of systematic reviews. Int J Qual Health Care. 2005 Apr;17(2):141–6. doi: 10.1093/intqhc/mzi016. http://intqhc.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=15665066mzi016 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
