

The neurogenic bladder: medical treatment
- PMID: 18095004
- PMCID: PMC2275777
- DOI: 10.1007/s00467-007-0691-z
The neurogenic bladder: medical treatment
Abstract
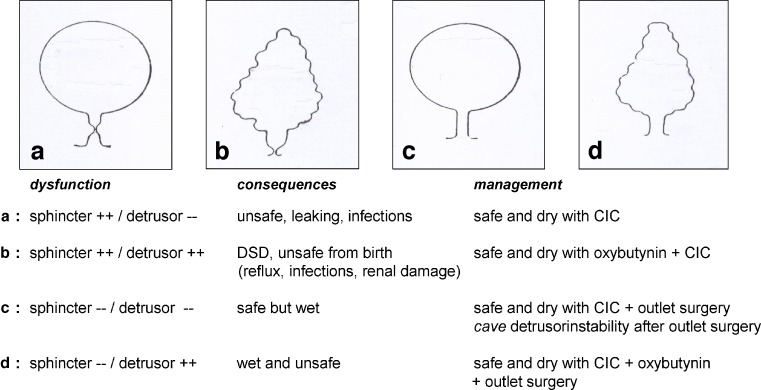
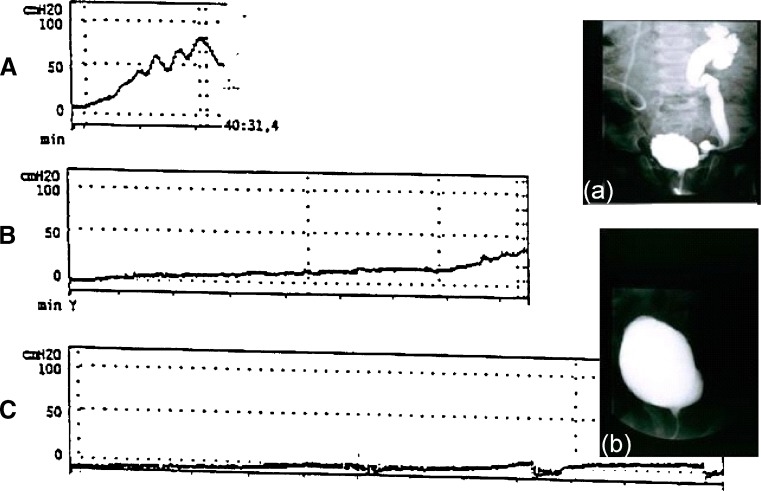
Neurogenic bladder sphincter dysfunction (NBSD) can cause severe and irreversible renal damage and bladder-wall destruction years before incontinence becomes an issue. Therefore, the first step in adequate management is to recognize early the bladder at risk for upper- and lower-tract deterioration and to start adequate medical treatment proactively. Clean intermittent catheterization combined with anticholinergics (oral or intravesical) is the standard therapy for NBSD. Early institution of such treatment can prevent both renal damage and secondary bladder-wall changes, thereby potentially improving long-term outcomes. In children with severe side effects or with insufficient suppression of detrusor overactivity despite maximal dosage of oral oxybutynin, intravesical instillation is an effective alternative. Intravesical instillation eliminates systemic side effects by reducing the first-pass metabolism and, compared with oral oxybutynin, intravesical oxybutynin is a more potent and long-acting detrusor suppressor. There is growing evidence that with early adequate treatment, kidneys are saved and normal bladder growth can be achieved in children so they will no longer need surgical bladder augmentation to achieve safe urinary continence in adolescence and adulthood.
Figures
References
-
- Lapides J, Diokno AC, Silber SJ, Lowe BS. Clean intermittent self-catheterization in the treatment of urinary tract disease. J Urol. 1972;107:458–461. - PubMed
-
- McGuire EJ, Woodside JR, Bordin TA, Weiss RM. Prognostic value of urodynamic testing in myelodysplastic patients. J Urol. 1981;136:205–209. - PubMed
-
- Bauer SB, Hallet M, Khoshbin S, Lebowitz RL, Winston KR, Gibson S, Colodny AH, Retik AB. Predictive value of urodynamic evaluation in newborns with myelodysplasia. JAMA. 1984;252:650–652. - PubMed
-
- Sidi AA, Peng W, Gonzalez R. Vesicoureteral reflux in children with myelodysplasia: natural history and results of treatment. J Urol. 1986;136:329–331. - PubMed
-
- Smith ED. Urinary prognosis in spina bifida. J Urol. 1972;108:815–817. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
